Department of Reproductive Medicine and Gynaecology, University Medical Centre Utrecht, University of Utrecht, Utrecht, The Netherlands.
BMC Womens Health. 2012 Sep 18;12:29. doi: 10.1186/1472-6874-12-29.
Costs of in vitro fertilisation (IVF) are high, which is partly due to the use of follicle stimulating hormone (FSH). FSH is usually administered in a standard dose. However, due to differences in ovarian reserve between women, ovarian response also differs with potential negative consequences on pregnancy rates. A Markov decision-analytic model showed that FSH dose individualisation according to ovarian reserve is likely to be cost-effective in women who are eligible for IVF. However, this has never been confirmed in a large randomised controlled trial (RCT). The aim of the present study is to assess whether an individualised FSH dose regime based on an ovarian reserve test (ORT) is more cost-effective than a standard dose regime.
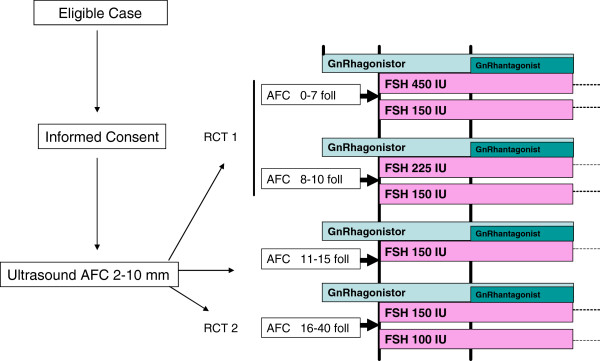
METHODS/DESIGN: Multicentre RCT in subfertile women indicated for a first IVF or intracytoplasmic sperm injection cycle, who are aged < 44 years, have a regular menstrual cycle and no major abnormalities at transvaginal sonography. Women with polycystic ovary syndrome, endocrine or metabolic abnormalities and women undergoing IVF with oocyte donation, will not be included. Ovarian reserve will be assessed by measuring the antral follicle count. Women with a predicted poor response or hyperresponse will be randomised for a standard versus an individualised FSH regime (150 IU/day, 225-450 IU/day and 100 IU/day, respectively). Participants will undergo a maximum of three stimulation cycles during maximally 18 months. The primary study outcome is the cumulative ongoing pregnancy rate resulting in live birth achieved within 18 months after randomisation. Secondary outcomes are parameters for ovarian response, multiple pregnancies, number of cycles needed per live birth, total IU of FSH per stimulation cycle, and costs. All data will be analysed according to the intention-to-treat principle. Cost-effectiveness analysis will be performed to assess whether the health and associated economic benefits of individualised treatment of subfertile women outweigh the additional costs of an ORT.
The results of this study will be integrated into a decision model that compares cost-effectiveness of the three dose-adjustment strategies to a standard dose strategy. The study outcomes will provide scientific foundation for national and international guidelines.
NTR2657.
体外受精(IVF)的成本很高,部分原因是使用了卵泡刺激素(FSH)。FSH 通常以标准剂量给药。然而,由于女性卵巢储备的差异,卵巢反应也不同,可能对妊娠率产生负面影响。一项马尔可夫决策分析模型显示,对于有资格接受 IVF 的女性,根据卵巢储备情况对 FSH 剂量进行个体化可能具有成本效益。然而,这从未在大型随机对照试验(RCT)中得到证实。本研究的目的是评估基于卵巢储备测试(ORT)的个体化 FSH 剂量方案是否比标准剂量方案更具成本效益。
方法/设计:在有生育能力的女性中进行的多中心 RCT,这些女性适合进行第一次 IVF 或胞浆内精子注射周期,年龄<44 岁,月经周期规律,经阴道超声检查无明显异常。多囊卵巢综合征、内分泌或代谢异常以及接受供卵 IVF 的女性将不包括在内。卵巢储备将通过测量窦卵泡计数来评估。预测反应不良或高反应的女性将被随机分为标准与个体化 FSH 方案(分别为 150IU/天、225-450IU/天和 100IU/天)。参与者将在最多 18 个月内进行最多 3 个刺激周期。主要研究结果是在随机分组后 18 个月内活产的累积持续妊娠率。次要结果是卵巢反应、多胎妊娠、每活产所需周期数、每个刺激周期的 FSH 总 IU 以及成本的参数。所有数据将根据意向治疗原则进行分析。成本效益分析将用于评估对生育能力低下的女性进行个体化治疗的健康和相关经济效益是否超过 ORT 的额外成本。
本研究的结果将纳入一个决策模型,该模型将比较三种剂量调整策略与标准剂量策略的成本效益。研究结果将为国家和国际指南提供科学依据。
NTR2657。