Zheng Haiyan, Chen Shiping, Du Hongzi, Ling Jiawei, Wu Yixuan, Liu Haiying, Liu Jianqiao
Center for Reproductive Medicine, Key Laboratory for Reproductive Medicine of Guangdong Province, Key Laboratory for Major Obstetric Diseases of Guangdong Province, Key Laboratory of Reproduction and Genetics of Guangdong Higher Education Institutes, Third Affiliated Hospital of Guangzhou Medical University, Guangzhou, Republic of China.
Medicine (Baltimore). 2017 Mar;96(13):e6495. doi: 10.1097/MD.0000000000006495.
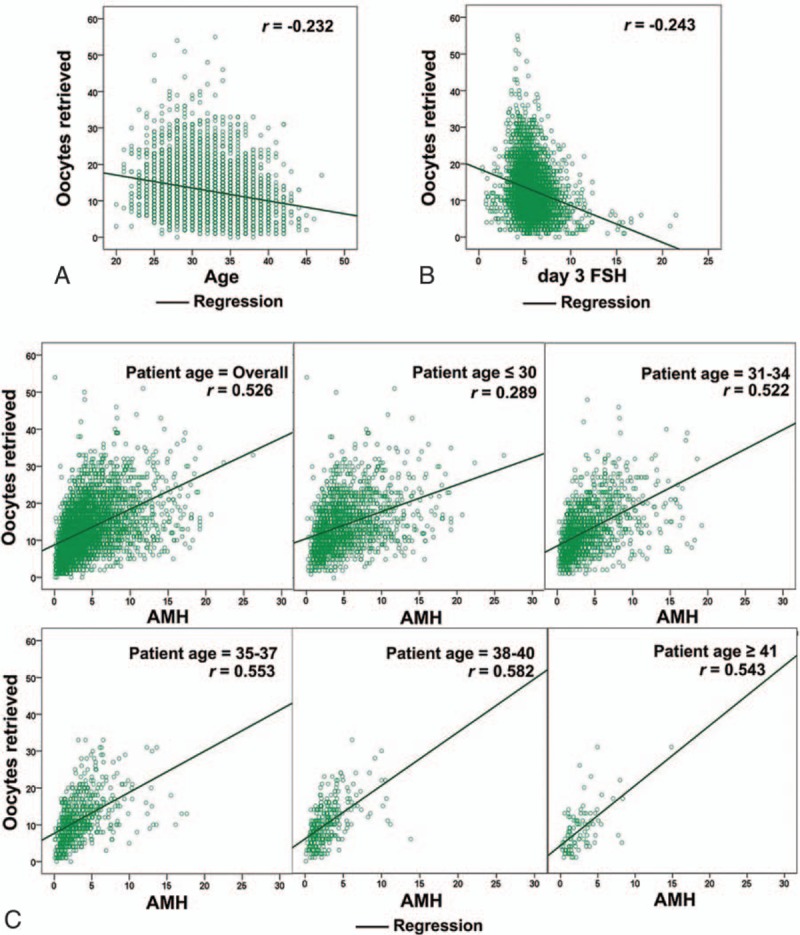
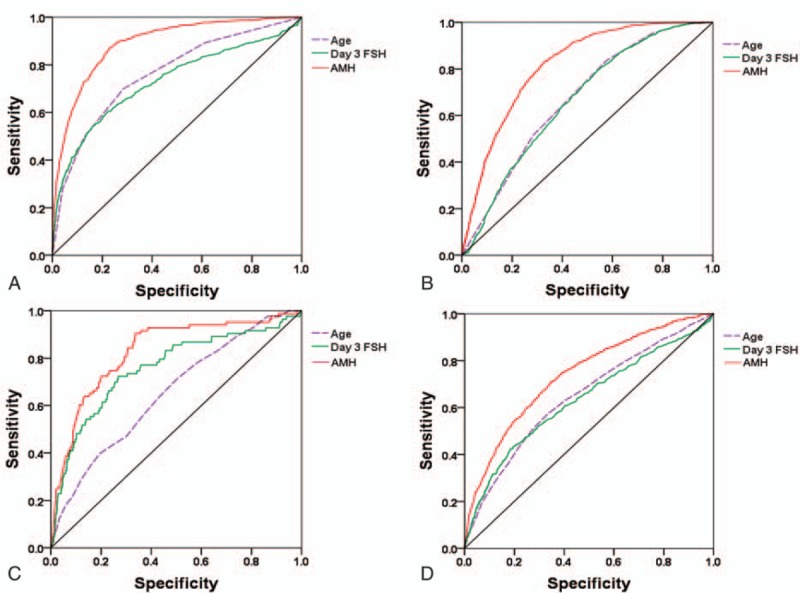
The predictive value of anti-Müllerian hormone (AMH) in Chinese women undergoing in vitro fertilization (IVF) treatment is data deficient. To determine the attributes of AMH in IVF, oocyte yield, cycle cancellation, and pregnancy outcomes were analyzed. All patients initiating their first IVF cycle with gonadotropin-releasing hormone agonist treatment in our center from October 2013 through December 2014 were included, except patients diagnosed with polycystic ovarian syndrome. Serum samples collected prior to IVF treatment were used to determine serum AMH levels. A total of 4017 continuous cycles were analyzed. The AMH level was positively correlated with the number of oocytes retrieved. Overall, AMH was significantly correlated with risk of cycle cancellation, poor ovarian response (POR, 3, or fewer oocytes retrieved) and high response (>15 oocytes), with an area under the curve (AUC) of 0.83, 0.89, and 0.82 respectively. An AMH cutoff of 0.6 ng/mL had a sensitivity of 54.0% and a specificity of 90.0% for the prediction of cycle cancellation, and cutoff of 0.8 ng/mL with a sensitivity of 55.0% and a specificity of 94.0% for the prediction of POR. Compared with AMH >2.0 ng/mL, patients with AMH < 0.6 ng/mL had a 53.6-fold increased risk of cancellation (P < 0.001), and AMH <0.80 ng/mL were 17.5 times more likely to experience POR (P < 0.001). However, AMH was less predictive of pregnancy and live birth, with AUCs of 0.55 and 0.53, respectively. Clinical pregnancy rate, ongoing pregnancy rate, and live birth rate per retrieval according to the AMH level (≤0.40, 0.41-0.60, 0.61-0.80, 0.81-1.00, 1.01-1.50, 1.51-2.00, and >2.00 ng/mL) showed no significant differences. Even with AMH≤0.4 ng/mL, 50.0% of all the patients achieved pregnancy and 34.8% of patients achieved live birth after transfer. Our results suggested that AMH is a fairly robust metric for the prediction of cycle cancellation and oocyte yield for Chinese women, but it is a relatively poor test for prediction of pregnancy outcomes. Patients with low levels of AMH still can achieve reasonable treatment outcomes and low AMH levels in isolation do not represent an appropriate marker for withholding fertility treatment.
抗苗勒管激素(AMH)在中国接受体外受精(IVF)治疗的女性中的预测价值数据不足。为了确定IVF中AMH的属性,分析了卵母细胞产量、周期取消率和妊娠结局。纳入了2013年10月至2014年12月在本中心开始首个使用促性腺激素释放激素激动剂治疗的IVF周期的所有患者,但不包括被诊断为多囊卵巢综合征的患者。IVF治疗前采集的血清样本用于测定血清AMH水平。共分析了4017个连续周期。AMH水平与回收的卵母细胞数量呈正相关。总体而言,AMH与周期取消风险、卵巢低反应(POR,回收3个或更少卵母细胞)和高反应(>15个卵母细胞)显著相关,曲线下面积(AUC)分别为0.83、0.89和0.82。AMH截断值为0.6 ng/mL时,预测周期取消的敏感性为54.0%,特异性为90.0%;截断值为0.8 ng/mL时,预测POR的敏感性为55.0%,特异性为94.0%。与AMH>2.0 ng/mL的患者相比,AMH<0.6 ng/mL的患者取消周期的风险增加了53.6倍(P<0.001),AMH<0.80 ng/mL的患者发生POR的可能性高17.5倍(P<0.001)。然而,AMH对妊娠和活产的预测性较差,AUC分别为0.55和0.53。根据AMH水平(≤0.40、0.41 - 0.60、0.61 - 0.80、0.81 - 1.00、1.01 - 1.50、1.51 - 2.00和>2.00 ng/mL)的每次取卵的临床妊娠率、持续妊娠率和活产率无显著差异。即使AMH≤0.4 ng/mL,所有患者中有50.0%实现了妊娠,34.8%的患者移植后实现了活产。我们的结果表明,AMH是预测中国女性周期取消和卵母细胞产量的一个相当可靠的指标,但它对妊娠结局的预测性相对较差。AMH水平低的患者仍可获得合理的治疗结果,孤立的低AMH水平并不代表停止生育治疗的合适指标。