African Medical and Research Foundation, Nairobi, Kenya.
Malar J. 2012 Sep 25;11:334. doi: 10.1186/1475-2875-11-334.
Effective case management of malaria requires prompt diagnosis and treatment within 24 hours. Home-based management of malaria (HMM) improves access to treatment for populations with limited access to health facilities. In Senegal, an HMM pilot study in 2008 demonstrated the feasibility of integrated use of RDTs and ACT in remote villages by volunteer Home Care Providers (HCP). Scale-up of the strategy began in 2009, reaching 408 villages in 2009 and 861 villages in 2010. This paper reports the results of the scale-up in the targeted communities and the impact of the strategy on malaria in the formal health sector.
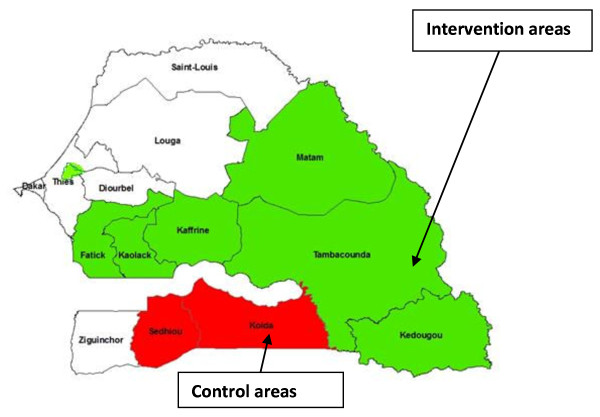
Data reported by the HCPs were used to assess their performance in 2009 and 2010, while routine malaria morbidity and mortality data were used to assess the impact of the HMM programme. Two high transmission regions where HMM was not implemented until 2010 were used as a comparison.
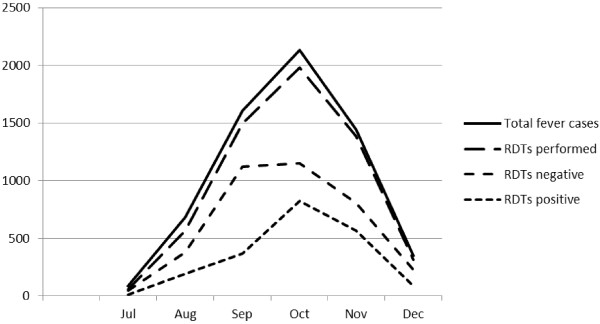
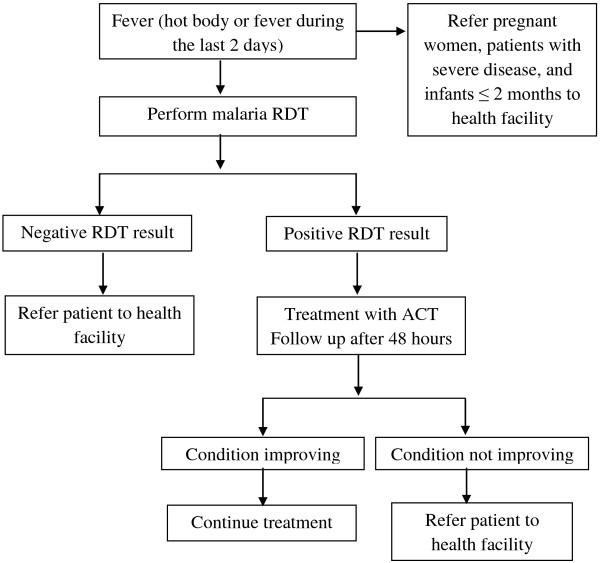
From July 2009 through May 2010, 12582 suspected cases were managed by HCPs, 93% (11672) of whom were tested with an RDT. Among those tested, 37% (4270) had a positive RDT, 97% (4126) of whom were reported treated and cured. Home care providers referred 6871 patients to health posts for management: 6486 with a negative RDT, 119 infants < 2 months, 105 pregnant women, and 161 severe cases. There were no deaths among these patients. In 2009 compared to 2008, incidence of suspected and confirmed malaria cases, all hospitalizations and malaria-related hospitalizations decreased in both intervention and comparison regions. Incidence of in-hospital deaths due to malaria decreased by 62.5% (95% CI 43.8-81.2) in the intervention regions, while the decrease in comparison regions was smaller and not statistically significant.
Home-based management of malaria including diagnosis with RDT and treatment based on test results is a promising strategy to improve the access of remote populations to prompt and effective management of uncomplicated malaria and to decrease mortality due to malaria. When scaled-up to serve remote village communities in the regions of Senegal with the highest malaria prevalence, home care providers demonstrated excellent adherence to guidelines, potentially contributing to a decrease in hospital deaths attributed to malaria.
有效管理疟疾需要在 24 小时内进行及时诊断和治疗。家庭为基础的疟疾管理(HMM)改善了那些难以获得卫生服务人群的治疗途径。在塞内加尔,2008 年的一项 HMM 试点研究表明,志愿家庭护理提供者(HCP)可以在偏远村庄中综合使用 RDT 和 ACT。该战略于 2009 年开始扩大规模,2009 年覆盖了 408 个村庄,2010 年覆盖了 861 个村庄。本文报告了该战略在目标社区的扩展结果以及该战略对正规卫生部门疟疾的影响。
利用 HCP 报告的数据评估他们在 2009 年和 2010 年的表现,同时利用常规疟疾发病率和死亡率数据评估 HMM 规划的影响。两个高传播地区直到 2010 年才实施 HMM,将其作为比较。
2009 年 7 月至 2010 年 5 月,12582 例疑似病例由 HCP 管理,其中 93%(11672 例)接受了 RDT 检测。在接受检测的病例中,37%(4270 例)的 RDT 检测结果呈阳性,其中 97%(4126 例)报告已接受治疗并治愈。HCP 将 6871 名患者转诊至卫生所进行治疗:6486 例 RDT 检测结果为阴性,119 名 2 个月以下婴儿,105 名孕妇和 161 名重症病例。这些患者中没有死亡病例。与 2008 年相比,在干预和对照地区,疑似和确诊疟疾病例的发病率、所有住院病例和疟疾相关住院病例均有所下降。干预地区因疟疾住院死亡的发病率下降了 62.5%(95%CI 43.8-81.2),而对照地区的降幅较小且无统计学意义。
包括使用 RDT 进行诊断和根据检测结果进行治疗的家庭为基础的疟疾管理是一种很有前途的策略,可以改善偏远地区人群获得及时有效的治疗机会,减少疟疾导致的死亡率。当该战略在塞内加尔疟疾流行率最高的地区扩展到服务偏远村庄社区时,家庭护理提供者严格遵守了指导方针,这可能有助于降低归因于疟疾的住院死亡率。