National Heart, Lung, and Blood Institute's Framingham Heart Study, Center for Population Studies Framingham, MA, USA.
Lancet. 2012 Nov 10;380(9854):1662-73. doi: 10.1016/S0140-6736(12)61350-6. Epub 2012 Sep 24.
Chronic kidney disease is characterised by low estimated glomerular filtration rate (eGFR) and high albuminuria, and is associated with adverse outcomes. Whether these risks are modified by diabetes is unknown.
We did a meta-analysis of studies selected according to Chronic Kidney Disease Prognosis Consortium criteria. Data transfer and analyses were done between March, 2011, and June, 2012. We used Cox proportional hazards models to estimate the hazard ratios (HR) of mortality and end-stage renal disease (ESRD) associated with eGFR and albuminuria in individuals with and without diabetes.
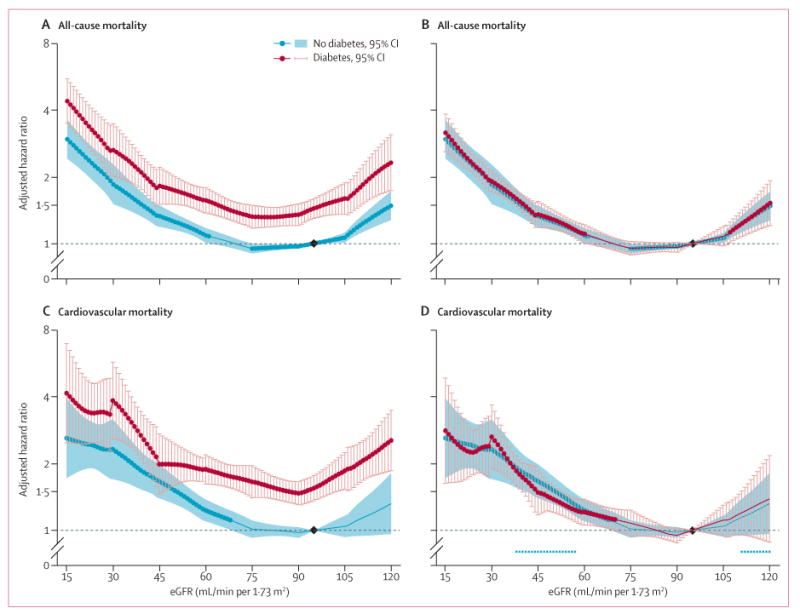
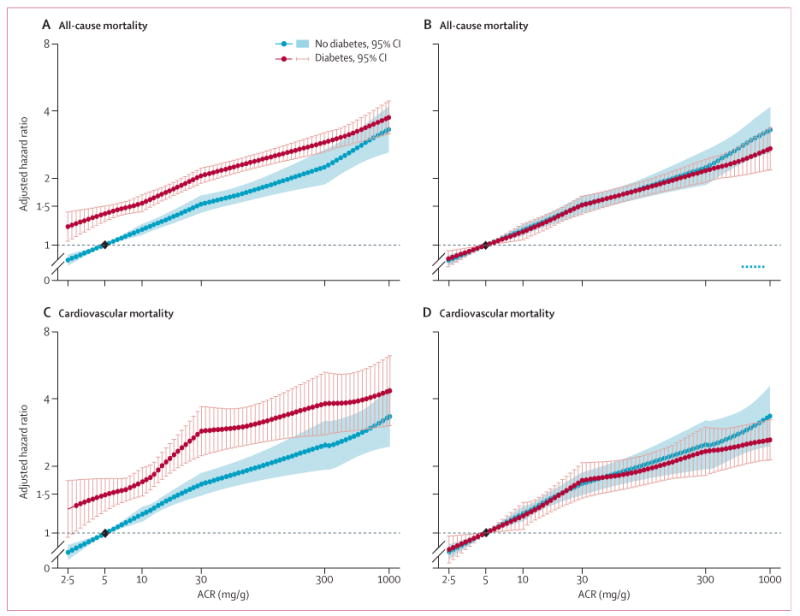
We analysed data for 1,024,977 participants (128,505 with diabetes) from 30 general population and high-risk cardiovascular cohorts and 13 chronic kidney disease cohorts. In the combined general population and high-risk cohorts with data for all-cause mortality, 75,306 deaths occurred during a mean follow-up of 8·5 years (SD 5·0). In the 23 studies with data for cardiovascular mortality, 21,237 deaths occurred from cardiovascular disease during a mean follow-up of 9·2 years (SD 4·9). In the general and high-risk cohorts, mortality risks were 1·2-1·9 times higher for participants with diabetes than for those without diabetes across the ranges of eGFR and albumin-to-creatinine ratio (ACR). With fixed eGFR and ACR reference points in the diabetes and no diabetes groups, HR of mortality outcomes according to lower eGFR and higher ACR were much the same in participants with and without diabetes (eg, for all-cause mortality at eGFR 45 mL/min per 1·73 m(2) [vs 95 mL/min per 1·73 m(2)], HR 1·35; 95% CI 1·18-1·55; vs 1·33; 1·19-1·48 and at ACR 30 mg/g [vs 5 mg/g], 1·50; 1·35-1·65 vs 1·52; 1·38-1·67). The overall interactions were not significant. We identified much the same findings for ESRD in the chronic kidney disease cohorts.
Despite higher risks for mortality and ESRD in diabetes, the relative risks of these outcomes by eGFR and ACR are much the same irrespective of the presence or absence of diabetes, emphasising the importance of kidney disease as a predictor of clinical outcomes.
US National Kidney Foundation.
慢性肾脏病的特征是肾小球滤过率(eGFR)估算值低和白蛋白尿高,并与不良结局相关。这些风险是否因糖尿病而改变尚不清楚。
我们根据慢性肾脏病预后联盟的标准,对选定的研究进行了荟萃分析。数据传输和分析于 2011 年 3 月至 2012 年 6 月进行。我们使用 Cox 比例风险模型来估计患有和不患有糖尿病的个体的死亡率和终末期肾病(ESRD)与 eGFR 和白蛋白尿相关的风险比(HR)。
我们分析了来自 30 个普通人群和高危心血管队列以及 13 个慢性肾脏病队列的 1024977 名参与者的数据(128505 名患有糖尿病)。在具有全因死亡率数据的普通人群和高危合并队列中,在平均 8.5 年(SD 5.0)的随访中发生了 75306 例死亡。在具有心血管死亡率数据的 23 项研究中,在平均 9.2 年(SD 4.9)的随访中有 21237 例死于心血管疾病。在普通人群和高危人群中,患有糖尿病的参与者的死亡率风险比无糖尿病参与者高出 1.2-1.9 倍,在 eGFR 和白蛋白/肌酐比值(ACR)的范围内。在糖尿病和无糖尿病组中以固定的 eGFR 和 ACR 参考点,死亡率结果的 HR 依据较低的 eGFR 和较高的 ACR 在有和没有糖尿病的参与者中大致相同(例如,在 eGFR 为 45 mL/min/1.73 m²[与 95 mL/min/1.73 m²相比]时,HR 为 1.35;95%CI 为 1.18-1.55;与 1.33;1.19-1.48 和在 ACR 为 30 mg/g[与 5 mg/g 相比]时,1.50;1.35-1.65 与 1.52;1.38-1.67)。总体交互作用不显著。我们在慢性肾脏病队列中发现了 ESRD 的大致相同的发现。
尽管糖尿病患者的死亡率和 ESRD 风险较高,但这些结果的相对风险与 eGFR 和 ACR 大致相同,无论是否存在糖尿病,这都强调了肾脏疾病作为临床结局预测因素的重要性。
美国国家肾脏基金会。