Department of Primary Care Health Sciences, Radcliffe Observatory Quarter, Oxford OX2 6GG, UK.
BMJ. 2012 Sep 25;345:e6144. doi: 10.1136/bmj.e6144.
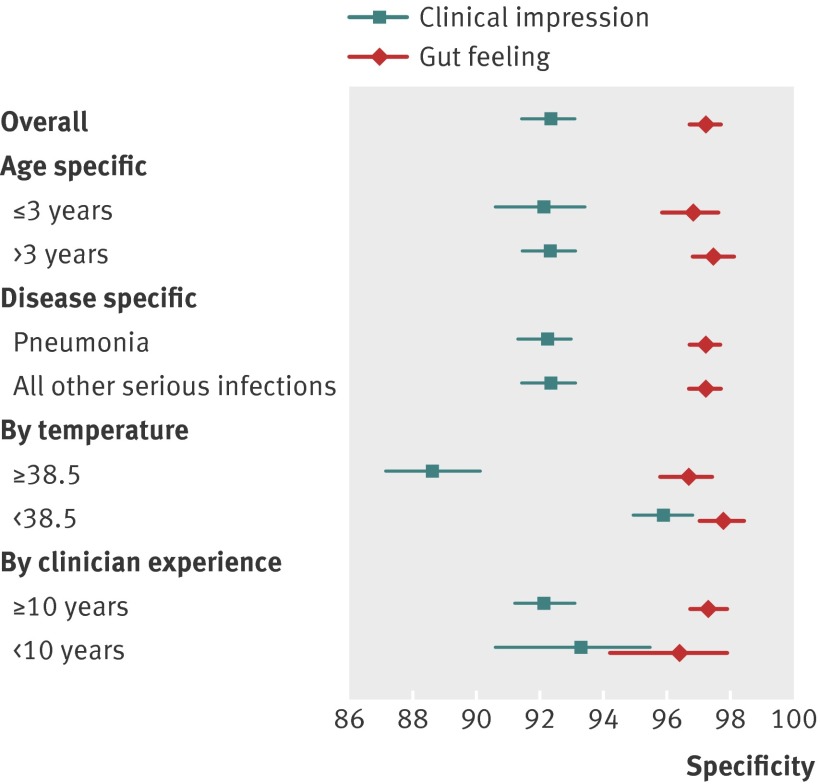
To investigate the basis and added value of clinicians' "gut feeling" that infections in children are more serious than suggested by clinical assessment.
Observational study.
Primary care setting, Flanders, Belgium.
Consecutive series of 3890 children and young people aged 0-16 years presenting in primary care.
Presenting features, clinical assessment, doctors' intuitive response at first contact with children in primary care, and any subsequent diagnosis of serious infection determined from hospital records.
Of the 3369 children and young people assessed clinically as having a non-severe illness, six (0.2%) were subsequently admitted to hospital with a serious infection. Intuition that something was wrong despite the clinical assessment of non-severe illness substantially increased the risk of serious illness (likelihood ratio 25.5, 95% confidence interval 7.9 to 82.0) and acting on this gut feeling had the potential to prevent two of the six cases being missed (33%, 95% confidence interval 4.0% to 100%) at a cost of 44 false alarms (1.3%, 95% confidence interval 0.95% to 1.75%). The clinical features most strongly associated with gut feeling were the children's overall response (drowsiness, no laughing), abnormal breathing, weight loss, and convulsions. The strongest contextual factor was the parents' concern that the illness was different from their previous experience (odds ratio 36.3, 95% confidence interval 12.3 to 107).
A gut feeling about the seriousness of illness in children is an instinctive response by clinicians to the concerns of the parents and the appearance of the children. It should trigger action such as seeking a second opinion or further investigations. The observed association between intuition and clinical markers of serious infection means that by reflecting on the genesis of their gut feeling, clinicians should be able to hone their clinical skills.
探究临床医生“直觉”认为儿童感染比临床评估所提示的更为严重的依据和附加价值。
观察性研究。
比利时弗兰德斯的初级保健机构。
连续系列的 3890 名 0-16 岁的儿童和年轻人,他们在初级保健机构就诊。
表现特征、临床评估、医生在初级保健机构首次接触儿童时的直观反应,以及从医院记录中确定的任何后续严重感染诊断。
在 3369 名临床评估为非严重疾病的儿童和年轻人中,有 6 名(0.2%)随后因严重感染住院。尽管临床评估为非严重疾病,但直觉认为病情异常,这大大增加了严重疾病的风险(似然比 25.5,95%置信区间 7.9 至 82.0),而根据这种直觉采取行动有可能避免 6 例漏诊中的 2 例(33%,95%置信区间 4.0%至 100%),代价是 44 次误诊(1.3%,95%置信区间 0.95%至 1.75%)。与直觉最相关的临床特征是儿童的整体反应(困倦、不笑)、呼吸异常、体重减轻和抽搐。最强的背景因素是父母认为疾病与他们以前的经验不同(比值比 36.3,95%置信区间 12.3 至 107)。
医生对儿童疾病严重程度的直觉是一种本能反应,是对父母的担忧和儿童外表的反应。这应该促使他们采取行动,如寻求第二意见或进一步调查。观察到的直觉与严重感染的临床标志物之间的关联意味着,通过反思他们直觉的起源,医生应该能够磨练他们的临床技能。