Hughston Clinic, Columbus, Georgia.
Sports Health. 2010 Mar;2(2):147-55. doi: 10.1177/1941738109338359.
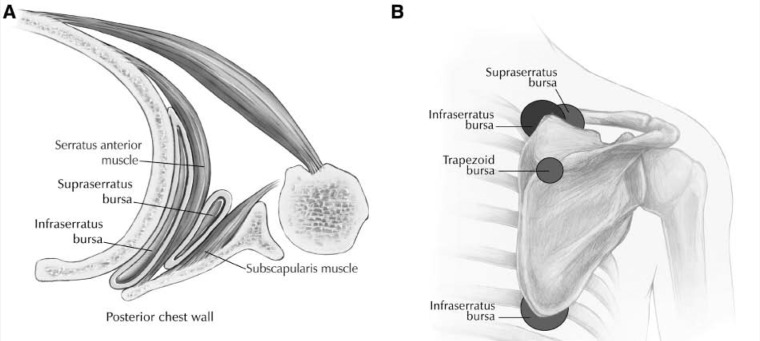
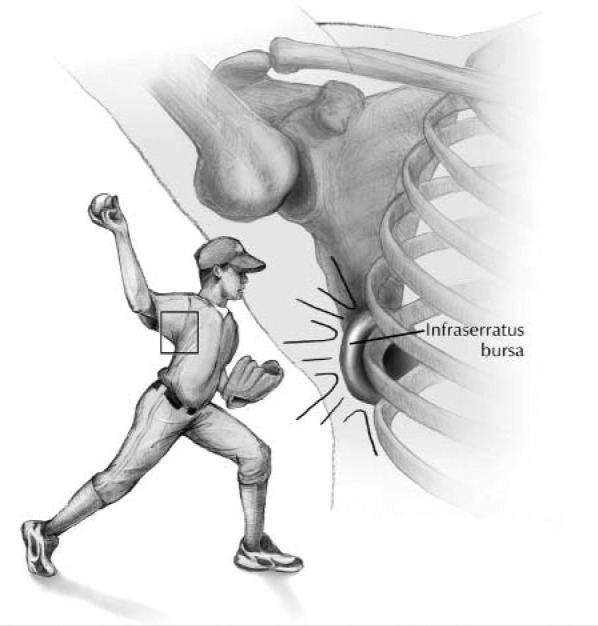
Symptomatic scapulothoracic bursitis and crepitus are disorders of the scapulothoracic articulation that are often poorly understood. They can be a source of persistent pain and dysfunction in the active overhead throwing athlete. It is important to distinguish between scapulothoracic bursitis and scapulothoracic crepitus. Scapulothoracic bursitis refers to inflammation of the bursae secondary to trauma or overuse owing to sports activities or work. Scapulothoracic crepitus is defined by a grinding, popping, or thumping sound or sensation secondary to abnormal scapulothoracic motion.
This article presents the causes, diagnosis, and management of these shoulder conditions in a manner that is relevant to clinicians, athletic trainers, and physical therapists, and it reviews relevant studies to determine the consensus on nonoperative treatment, as well as open and arthroscopic surgical treatment.
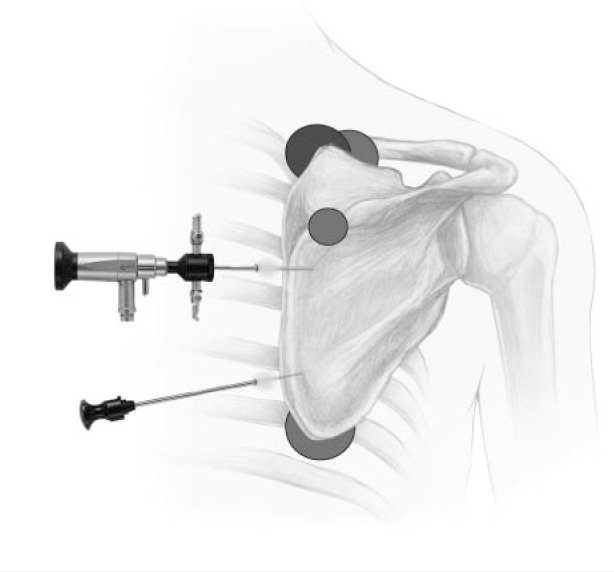
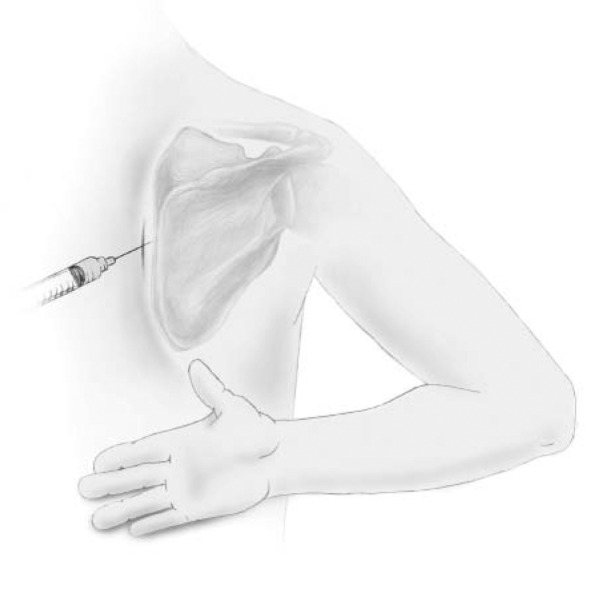
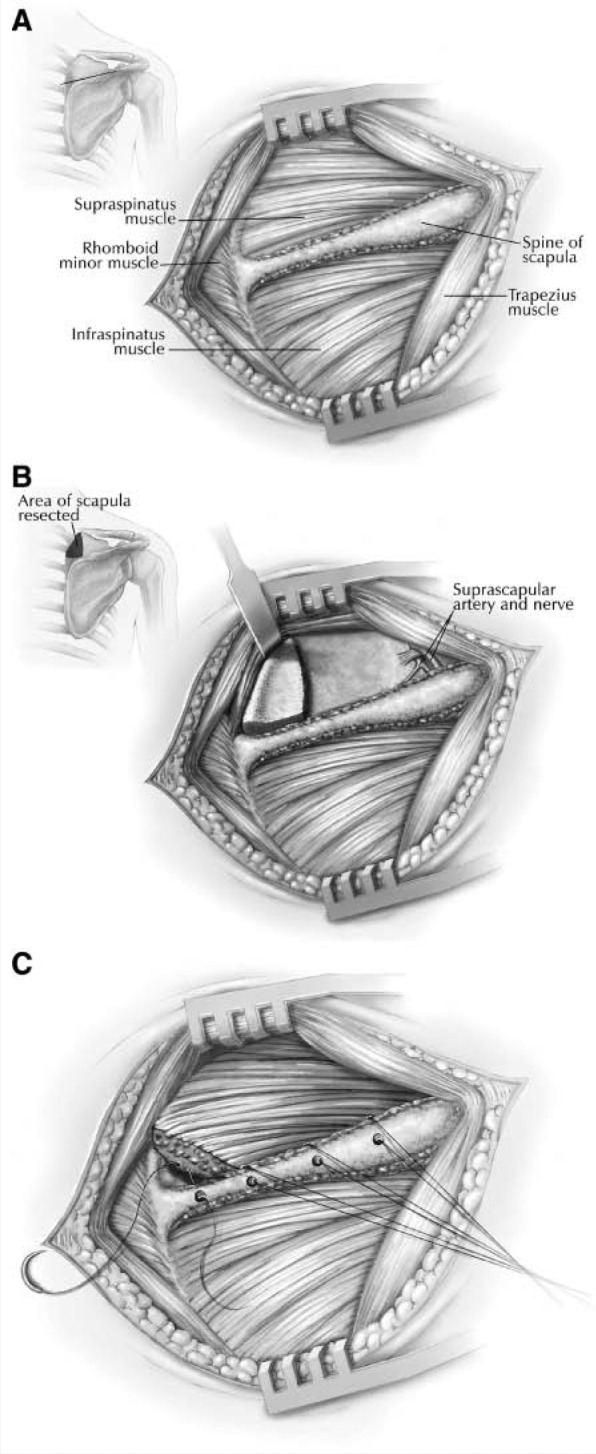
The causes of scapulothoracic bursitis and crepitus include direct or indirect trauma, overuse syndromes, glenohumeral joint dysfunction, osseous abnormalities, muscle atrophy or fibrosis, and idiopathic causes. Scapulothoracic bursitis and crepitus remain primarily clinical diagnoses; however, imaging studies or local injections may also be helpful. The initial treatment of scapulothoracic bursitis and scapulothoracic crepitus should be nonoperative. Surgical treatment options include partial scapulectomy or resection of the superomedial angle of the scapula, open bursal resection, and arthroscopic bursectomy. Despite the lack of agreement among orthopaedic surgeons concerning which procedure is best for treating symptomatic scapulothoracic bursitis and crepitus, most reports have demonstrated good to excellent outcomes in a significantly high percentage of patients.
Clearly, the best initial approach to these conditions is a nonoperative treatment plan that combines scapular strengthening, postural reeducation, and core strength endurance. The addition of local modalities, nonsteroidal anti- inflammatory drugs, and localized injections may also be helpful. If an appropriate trial of nonoperative management proves unsuccessful, surgical correction can produce good results.
症状性肩胛胸壁囊炎和弹响是肩胛胸关节的疾病,通常理解较差。它们可能是活动过顶投掷运动员持续疼痛和功能障碍的根源。区分肩胛胸囊炎和肩胛胸壁弹响很重要。肩胛胸囊炎是指由于创伤或过度使用(由于运动或工作)导致滑囊炎炎症。肩胛胸壁弹响是指由于肩胛胸运动异常而产生的摩擦、爆裂或砰砰声或感觉。
本文以与临床医生、运动训练师和物理治疗师相关的方式介绍了这些肩部疾病的病因、诊断和治疗,并回顾了相关研究,以确定非手术治疗以及开放和关节镜手术治疗的共识。
肩胛胸囊炎和弹响的原因包括直接或间接创伤、过度使用综合征、盂肱关节功能障碍、骨异常、肌肉萎缩或纤维化以及特发性原因。肩胛胸囊炎和弹响仍然主要是临床诊断;然而,影像学研究或局部注射也可能有帮助。肩胛胸囊炎和肩胛胸壁弹响的初始治疗应是非手术治疗。手术治疗选择包括肩胛下部分切除术或肩胛上内角切除术、开放滑囊切除术和关节镜下滑囊切除术。尽管矫形外科医生对治疗症状性肩胛胸囊炎和肩胛胸壁弹响的最佳手术方法存在分歧,但大多数报告显示,在很大比例的患者中,手术结果良好或优秀。
显然,这些疾病的最佳初始方法是结合肩胛强化、姿势再教育和核心力量耐力的非手术治疗计划。局部治疗、非甾体抗炎药和局部注射也可能有帮助。如果非手术治疗方案不成功,手术矫正可以取得良好效果。