Department of Renal Medicine, Royal Derby Hospital, Derby, United Kingdom.
PLoS One. 2012;7(11):e48580. doi: 10.1371/journal.pone.0048580. Epub 2012 Nov 2.
The high mortality rates that follow the onset of acute kidney injury (AKI) are well recognised. However, the mode of death in patients with AKI remains relatively under-studied, particularly in general hospitalised populations who represent the majority of those affected. We sought to describe the primary cause of death in a large group of prospectively identified patients with AKI.
All patients sustaining AKI at our centre between 1(st) October 2010 and 31(st) October 2011 were identified by real-time, hospital-wide, electronic AKI reporting based on the Acute Kidney Injury Network (AKIN) diagnostic criteria. Using this system we are able to generate a prospective database of all AKI cases that includes demographic, outcome and hospital coding data. For those patients that died during hospital admission, cause of death was derived from the Medical Certificate of Cause of Death.
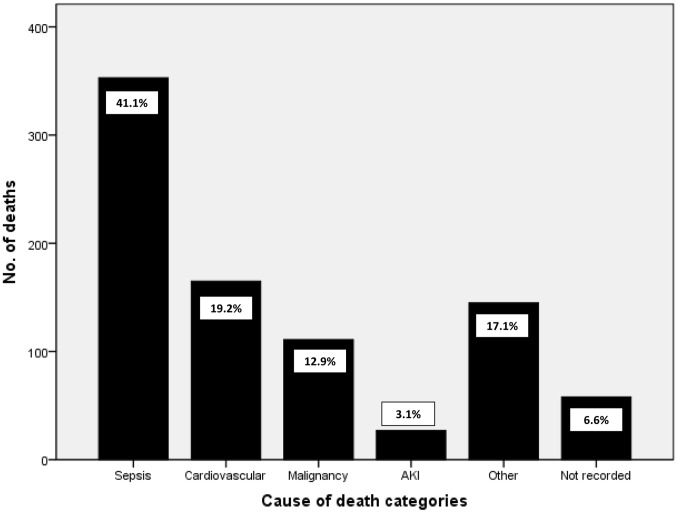
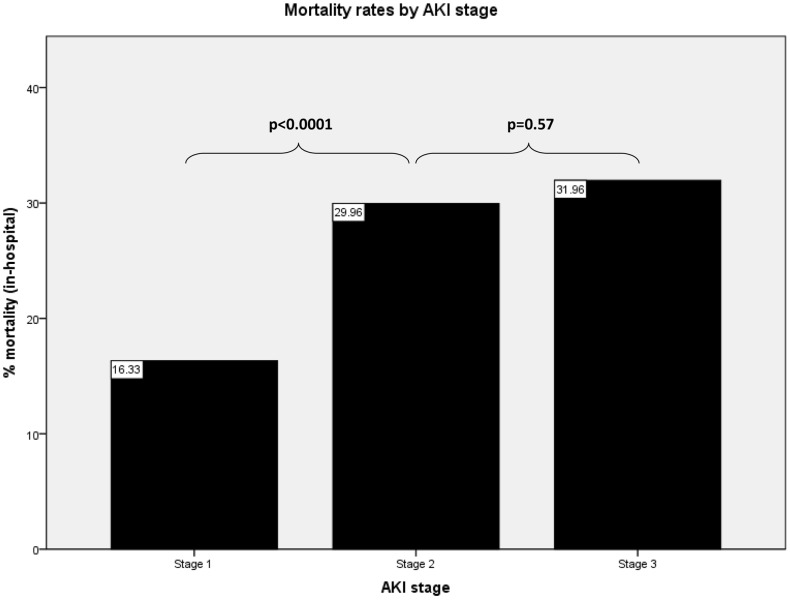
During the study period there were 3,930 patients who sustained AKI; 62.0% had AKI stage 1, 20.6% had stage 2 and 17.4% stage 3. In-hospital mortality rate was 21.9% (859 patients). Cause of death could be identified in 93.4% of cases. There were three main disease categories accounting for three quarters of all mortality; sepsis (41.1%), cardiovascular disease (19.2%) and malignancy (12.9%). The major diagnosis leading to sepsis was pneumonia, whilst cardiovascular death was largely a result of heart failure and ischaemic heart disease. AKI was the primary cause of death in only 3% of cases.
Mortality associated with AKI remains high, although cause of death is usually concurrent illness. Specific strategies to improve outcomes may therefore need to target not just the management of AKI but also the most relevant co-existing conditions.
急性肾损伤(AKI)发病后死亡率很高,这一点已得到广泛认可。然而,AKI 患者的死亡模式仍相对研究不足,特别是在代表大多数受影响人群的综合医院住院患者中。我们试图描述一组经前瞻性识别的 AKI 患者中大量患者的主要死亡原因。
我们通过基于急性肾损伤网络(AKIN)诊断标准的实时、全院范围的电子 AKI 报告系统,确定了我们中心在 2010 年 10 月 1 日至 2011 年 10 月 31 日期间发生的所有 AKI 患者。通过该系统,我们能够生成包含人口统计学、结果和医院编码数据的所有 AKI 病例的前瞻性数据库。对于住院期间死亡的患者,死因来自死亡原因的医疗证明。
在研究期间,共有 3930 名患者发生 AKI;62.0%为 AKI 1 期,20.6%为 AKI 2 期,17.4%为 AKI 3 期。住院死亡率为 21.9%(859 例)。在 93.4%的病例中可以确定死因。有三个主要疾病类别占所有死亡人数的四分之三;脓毒症(41.1%)、心血管疾病(19.2%)和恶性肿瘤(12.9%)。导致脓毒症的主要诊断是肺炎,而心血管死亡主要是心力衰竭和缺血性心脏病的结果。AKI 仅作为主要死因导致 3%的病例死亡。
尽管死亡原因通常是合并症,但 AKI 相关死亡率仍然很高。因此,改善预后的具体策略可能不仅需要针对 AKI 的治疗,还需要针对最相关的并存疾病。