Health Services Research Group, Centre for Geographic Medicine Research - Coast, Kenya Medical Research Institute/Wellcome Trust Research Programme, Nairobi, Kenya.
PLoS One. 2012;7(11):e47622. doi: 10.1371/journal.pone.0047622. Epub 2012 Nov 5.
The existing case fatality estimates of inpatient childhood pneumonia in developing countries are largely from periods preceding routine use of conjugate vaccines for infant immunization and such primary studies rarely explore hospital variations in mortality. We analysed case fatality rates of children admitted to nine Kenyan hospitals with pneumonia during the era of routine infant immunization with Hib conjugate vaccine to determine if significant variations exist between hospitals.
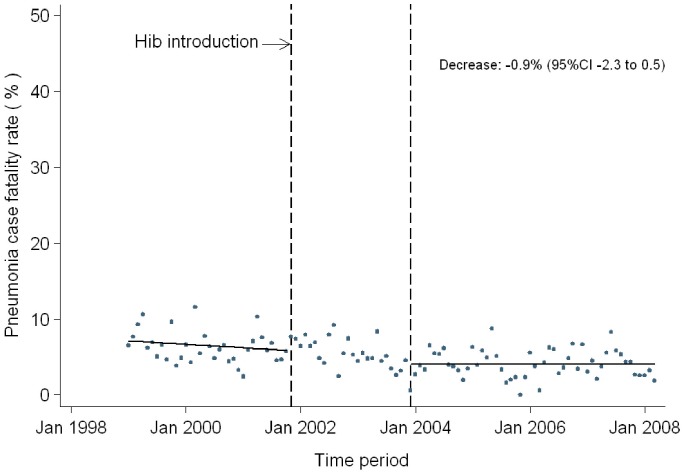
Pneumonia admissions and outcomes in paediatric wards are described using data collected over two time periods: a one-year period (2007-2008) in nine hospitals, and data from a 9.25-year period (1999-March 2008) in one of the participating hospitals. Hospital case fatality rates for inpatient pneumonia during 2007 to 2008 were modeled using a fixed effect binomial regression model with a logit link. Using an interrupted time series design, data from one hospital were analysed for trends in pneumonia mortality during the period between 1997 and March 2008.
Overall, 195 (5.9%) children admitted to all 9 hospitals with pneumonia from March 2007 to March 2008 died in hospital. After adjusting for child's sex, comorbidity, and hospital effect, mortality was significantly associated with child's age (p<0.001) and pneumonia severity (p<0.001). There was evidence of significant variations in mortality between hospitals (LR χ(2) =52.19; p<0.001). Pneumonia mortality remained stable in the periods before (trend -0.03, 95% CI -0.1 to 0.02) and after Hib introduction (trend 0.04, 95% CI -0.04 to 0.11).
There are important variations in hospital-pneumonia case fatality in Kenya and these variations are not attributed to temporal changes. Such variations in mortality are not addressed by existing epidemiological models and need to be considered in allocating resources to improve child health.
发展中国家现有的住院儿童肺炎病死率估算主要来自于在常规使用婴幼儿疫苗之前的时期,而这些初步研究很少探索医院间死亡率的差异。我们分析了在常规使用 Hib 结合疫苗为婴儿免疫的时代,肯尼亚 9 家医院因肺炎住院的儿童病死率,以确定医院间是否存在显著差异。
使用在两个时间段收集的数据描述儿科病房的肺炎入院和结局:9 家医院的一年期(2007-2008 年)和参与医院的 9.25 年(1999 年-2008 年 3 月)的数据。使用固定效应二项回归模型和对数链接,对 2007 年至 2008 年期间住院肺炎的医院病死率进行建模。使用中断时间序列设计,分析一家医院在 1997 年至 2008 年 3 月期间肺炎死亡率的趋势。
总体而言,2007 年 3 月至 2008 年 3 月期间,9 家医院因肺炎住院的 195 名儿童中有 5.9%死亡。在调整儿童性别、合并症和医院效果后,死亡率与儿童年龄(p<0.001)和肺炎严重程度(p<0.001)显著相关。医院间死亡率存在显著差异(LR χ(2) =52.19;p<0.001)。在 Hib 引入之前(趋势-0.03,95%CI-0.1 至 0.02)和之后(趋势 0.04,95%CI-0.04 至 0.11),肺炎死亡率均保持稳定。
肯尼亚医院间肺炎病死率存在重要差异,且这些差异与时间变化无关。现有的流行病学模型并未解决死亡率的这种差异,需要在分配资源以改善儿童健康时考虑到这一点。