Division of Pulmonary and Critical Care Medicine, San Francisco General Hospital, University of California San Francisco, San Francisco, California, USA.
PLoS One. 2012;7(11):e48599. doi: 10.1371/journal.pone.0048599. Epub 2012 Nov 6.
The clinical impact of Xpert MTB/RIF for tuberculosis (TB) diagnosis in high HIV-prevalence settings is unknown.
To determine the diagnostic accuracy and impact of Xpert MTB/RIF among high-risk TB suspects.
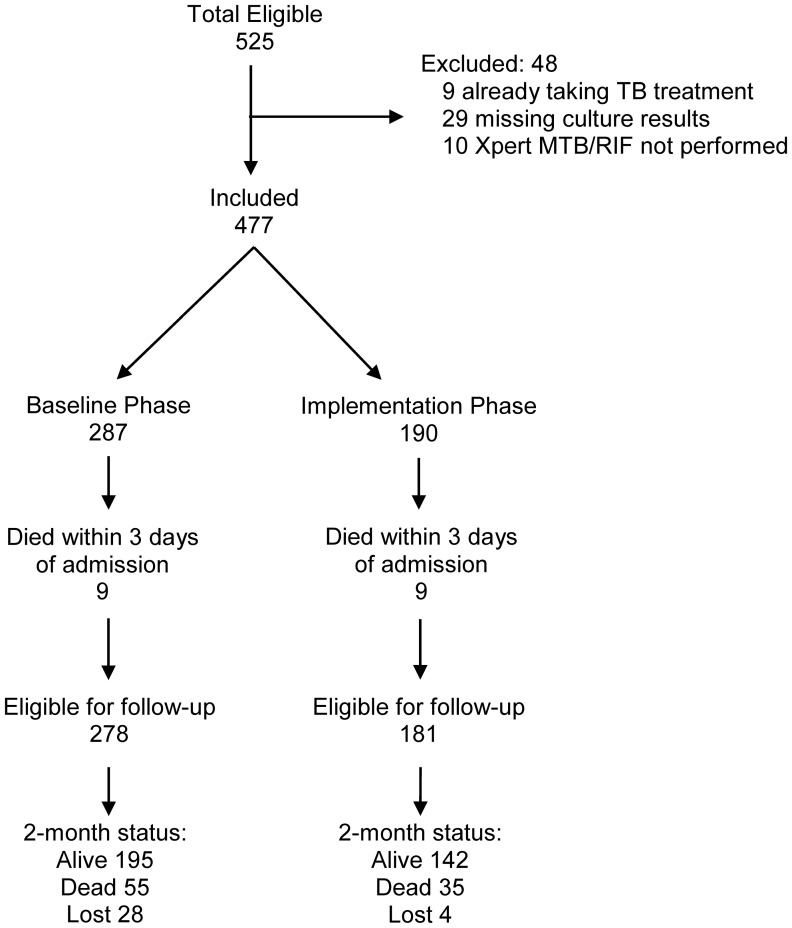
WE PROSPECTIVELY ENROLLED CONSECUTIVE, HOSPITALIZED, UGANDAN TB SUSPECTS IN TWO PHASES: baseline phase in which Xpert MTB/RIF results were not reported to clinicians and an implementation phase in which results were reported. We determined the diagnostic accuracy of Xpert MTB/RIF in reference to culture (solid and liquid) and compared patient outcomes by study phase.
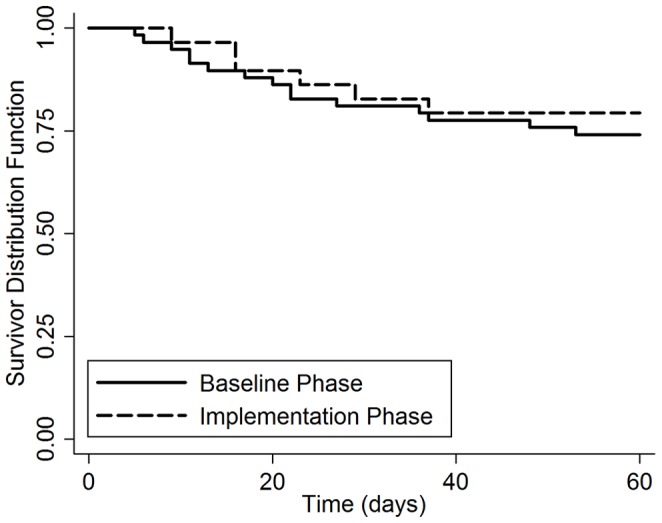
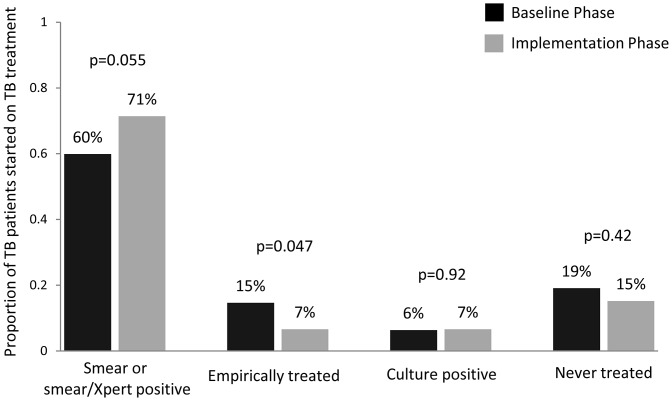
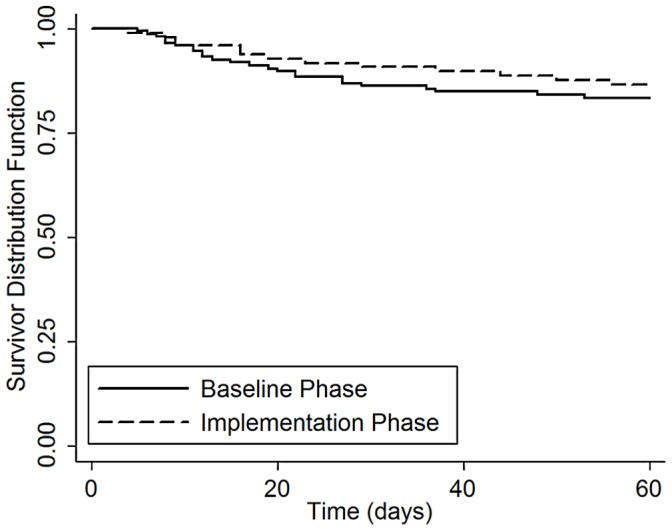
477 patients were included (baseline phase 287, implementation phase 190). Xpert MTB/RIF had high sensitivity (187/237, 79%, 95% CI: 73-84%) and specificity (190/199, 96%, 95% CI: 92-98%) for culture-positive TB overall, but sensitivity was lower (34/81, 42%, 95% CI: 31-54%) among smear-negative TB cases. Xpert MTB/RIF reduced median days-to-TB detection for all TB cases (1 [IQR 0-26] vs. 0 [IQR 0-1], p<0.001), and for smear-negative TB (35 [IQR 22-55] vs. 22 [IQR 0-33], p=0.001). However, median days-to-TB treatment was similar for all TB cases (1 [IQR 0-5] vs. 0 [IQR 0-2], p=0.06) and for smear-negative TB (7 [IQR 3-53] vs. 6 [IQR 1-61], p=0.78). Two-month mortality was also similar between study phases among 252 TB cases (17% vs. 14%, difference +3%, 95% CI: -21% to +27%, p=0.80), and among 87 smear-negative TB cases (28% vs. 22%, difference +6%, 95% CI: -34 to +46%, p=0.77).
Xpert MTB/RIF facilitated more accurate and earlier TB diagnosis, leading to a higher proportion of TB suspects with a confirmed TB diagnosis prior to hospital discharge in a high HIV/low MDR TB prevalence setting. However, our study did not detect a decrease in two-month mortality following implementation of Xpert MTB/RIF possibly because of insufficient powering, differences in empiric TB treatment rates, and disease severity between study phases.
Xpert MTB/RIF 检测对高 HIV 流行地区结核病(TB)诊断的临床影响尚不清楚。
确定 Xpert MTB/RIF 在高危 TB 疑似病例中的诊断准确性和影响。
我们前瞻性地招募了两阶段的连续住院乌干达 TB 疑似病例:基线阶段不向临床医生报告 Xpert MTB/RIF 结果,实施阶段报告结果。我们参考培养物(固体和液体)确定了 Xpert MTB/RIF 的诊断准确性,并比较了研究阶段的患者结局。
共纳入 477 例患者(基线阶段 287 例,实施阶段 190 例)。Xpert MTB/RIF 对所有培养阳性的 TB 总体具有较高的敏感性(187/237,79%,95%CI:73-84%)和特异性(190/199,96%,95%CI:92-98%),但在涂片阴性的 TB 病例中敏感性较低(34/81,42%,95%CI:31-54%)。Xpert MTB/RIF 缩短了所有 TB 病例的中位 TB 检测时间(1 [IQR 0-26] vs. 0 [IQR 0-1],p<0.001),以及涂片阴性的 TB 病例(35 [IQR 22-55] vs. 22 [IQR 0-33],p=0.001)。然而,所有 TB 病例的中位 TB 治疗时间相似(1 [IQR 0-5] vs. 0 [IQR 0-2],p=0.06),以及涂片阴性的 TB 病例(7 [IQR 3-53] vs. 6 [IQR 1-61],p=0.78)。在 252 例 TB 病例中,两个阶段的 2 个月死亡率也相似(17% vs. 14%,差异+3%,95%CI:-21%至+27%,p=0.80),以及 87 例涂片阴性的 TB 病例(28% vs. 22%,差异+6%,95%CI:-34%至+46%,p=0.77)。
Xpert MTB/RIF 有助于更准确和更早地诊断 TB,导致在高 HIV/低 MDR-TB 流行地区,在出院前有更高比例的 TB 疑似病例被确诊为 TB。然而,我们的研究没有发现 Xpert MTB/RIF 实施后两个月死亡率的降低,这可能是因为效力不足、经验性 TB 治疗率的差异以及两个研究阶段之间的疾病严重程度不同。