Kim Sun, Can Melike Hazal, Agizew Tefera B, Auld Andrew F, Balcells Maria Elvira, Bjerrum Stephanie, Dheda Keertan, Dorman Susan E, Esmail Aliasgar, Fielding Katherine, Garcia-Basteiro Alberto L, Hanrahan Colleen F, Kebede Wakjira, Kohli Mikashmi, Luetkemeyer Anne F, Mita Carol, Reeve Byron W P, Silva Denise Rossato, Sweeney Sedona, Theron Grant, Trajman Anete, Vassall Anna, Warren Joshua L, Yotebieng Marcel, Cohen Ted, Menzies Nicolas A
Department of Global Health and Population, Harvard T.H. Chan School of Public Health, Boston, MA, USA.
U.S. Centers for Disease Control and Prevention, Botswana.
medRxiv. 2024 Apr 8:2024.04.07.24305445. doi: 10.1101/2024.04.07.24305445.
Globally, over one-third of pulmonary tuberculosis (TB) disease diagnoses are made based on clinical criteria after a negative diagnostic test result. Understanding factors associated with clinicians' decisions to initiate treatment for individuals with negative test results is critical for predicting the potential impact of new diagnostics.
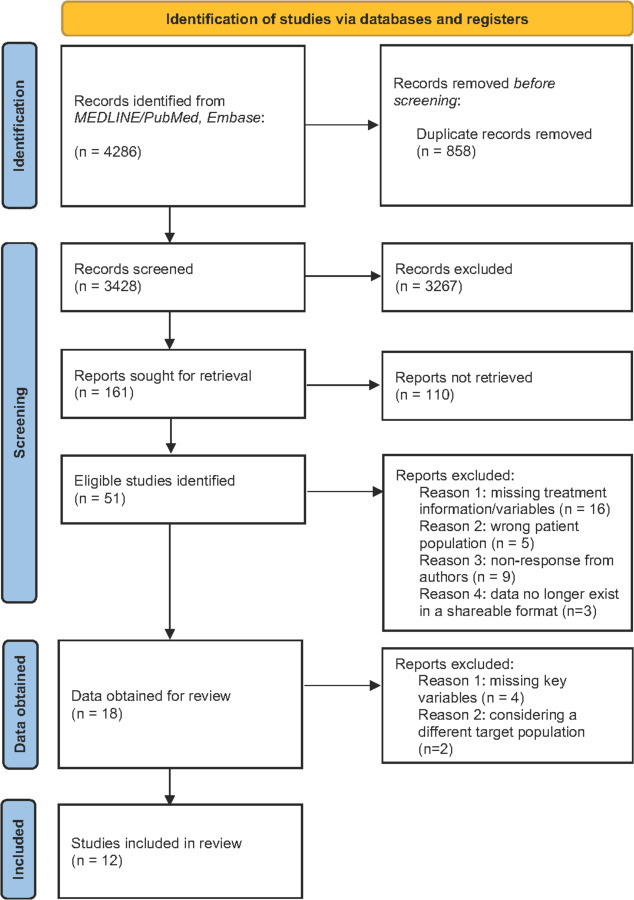
We performed a systematic review and individual patient data meta-analysis using studies conducted between January/2010 and December/2022 (PROSPERO: CRD42022287613). We included trials or cohort studies that enrolled individuals evaluated for TB in routine settings. In these studies participants were evaluated based on clinical examination and routinely-used diagnostics, and were followed for ≥1 week after the initial test result. We used hierarchical Bayesian logistic regression to identify factors associated with treatment initiation following a negative result on an initial bacteriological test (e.g., sputum smear microscopy, Xpert MTB/RIF).
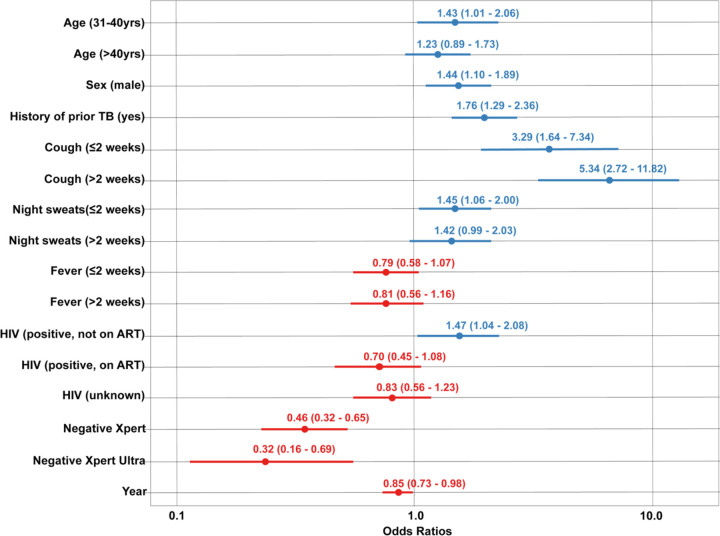
Multiple factors were positively associated with treatment initiation: male sex [adjusted Odds Ratio (aOR) 1.61 (1.31-1.95)], history of prior TB [aOR 1.36 (1.06-1.73)], reported cough [aOR 4.62 (3.42-6.27)], reported night sweats [aOR 1.50 (1.21-1.90)], and having HIV infection but not on ART [aOR 1.68 (1.23-2.32)]. Treatment initiation was substantially less likely for individuals testing negative with Xpert [aOR 0.77 (0.62-0.96)] compared to smear microscopy and declined in more recent years.
Multiple factors influenced decisions to initiate TB treatment despite negative test results. Clinicians were substantially less likely to treat in the absence of a positive test result when using more sensitive, PCR-based diagnostics.
在全球范围内,超过三分之一的肺结核(TB)疾病诊断是在诊断检测结果为阴性后根据临床标准做出的。了解与临床医生对检测结果为阴性的个体启动治疗的决定相关的因素,对于预测新诊断方法的潜在影响至关重要。
我们使用2010年1月至2022年12月期间开展的研究进行了一项系统评价和个体患者数据荟萃分析(国际前瞻性系统评价注册库:CRD42022287613)。我们纳入了在常规环境中对疑似结核病个体进行评估的试验或队列研究。在这些研究中,参与者通过临床检查和常规使用的诊断方法进行评估,并在初始检测结果后随访≥1周。我们使用分层贝叶斯逻辑回归来确定与初始细菌学检测(如痰涂片显微镜检查、Xpert MTB/RIF)结果为阴性后启动治疗相关的因素。
多个因素与治疗启动呈正相关:男性[调整优势比(aOR)1.61(1.31 - 1.95)]、既往结核病病史[aOR 1.36(1.06 - 1.73)]、报告有咳嗽症状[aOR 4.62(3.42 - 6.27)]、报告有盗汗症状[aOR 1.50(1.21 - 1.90)]以及感染了HIV但未接受抗逆转录病毒治疗[aOR 1.68(1.23 - 2.32)]。与涂片显微镜检查相比,Xpert检测结果为阴性的个体启动治疗的可能性显著降低[aOR 0.77(0.62 - 0.96)],且近年来呈下降趋势。
尽管检测结果为阴性,但多个因素影响了启动结核病治疗的决定。当使用更敏感的基于PCR的诊断方法时,如果检测结果为阴性,临床医生进行治疗的可能性会大幅降低。