Getting Better at Chronic Care Project, University of South Australia, School of Health Sciences, Cairns Diabetes Centre, 381 Sheridan St, North Cairns, QLD, 4870, Australia.
BMC Public Health. 2012 Nov 21;12:1017. doi: 10.1186/1471-2458-12-1017.
Prevalence and incidence of diabetes and other common comorbid conditions (hypertension, coronary heart disease, renal disease and chronic lung disease) are extremely high among Indigenous Australians. Recent measures to improve quality of preventive care in Indigenous community settings, while apparently successful at increasing screening and routine check-up rates, have shown only modest or little improvements in appropriate care such as the introduction of insulin and other scaled-up drug regimens in line with evidence-based guidelines, together with support for risk factor reduction. A new strategy is required to ensure high quality integrated family-centred care is available locally, with continuity and cultural safety, by community-based care coordinators with appropriate system supports.
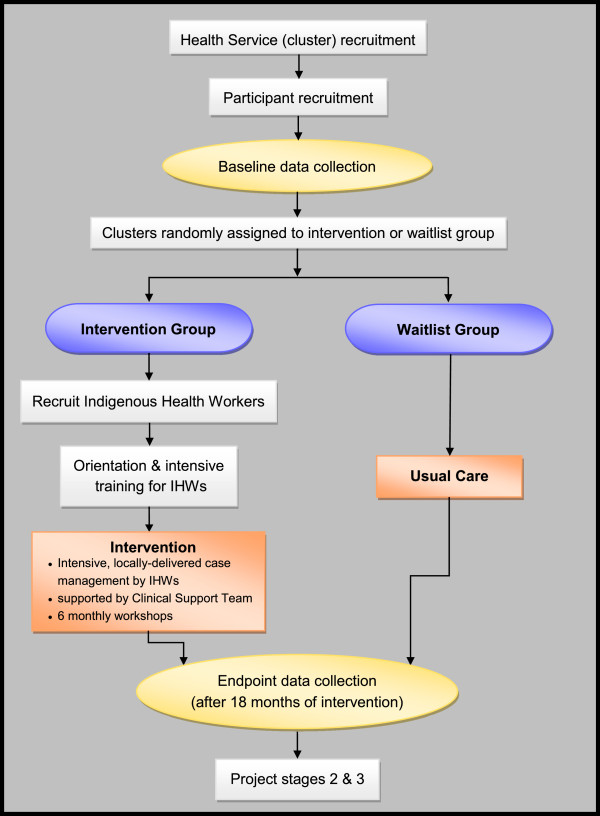
METHODS/DESIGN: The trial design is open parallel cluster randomised controlled trial. The objective of this pragmatic trial is to test the effectiveness of a model of health service delivery that facilitates integrated community-based, intensive chronic condition management, compared with usual care, in rural and remote Indigenous primary health care services in north Queensland. Participants are Indigenous adults (aged 18-65 years) with poorly controlled diabetes (HbA1c>=8.5) and at least one other chronic condition. The intervention is to employ an Indigenous Health Worker to case manage the care of a maximum caseload of 30 participants. The Indigenous Health Workers receive intensive clinical training initially, and throughout the study, to ensure they are competent to coordinate care for people with chronic conditions. The Indigenous Health Workers, supported by the local primary health care (PHC) team and an Indigenous Clinical Support Team, will manage care, including coordinating access to multidisciplinary team care based on best practice standards. Allocation by cluster to the intervention and control groups is by simple randomisation after participant enrolment. Participants in the control group will receive usual care, and will be wait-listed to receive a revised model of the intervention informed by the data analysis. The primary outcome is reduction in HbA1c measured at 18 months. Implementation fidelity will be monitored and a qualitative investigation (methods to be determined) will aim to identify elements of the model which may influence health outcomes for Indigenous people with chronic conditions.
This pragmatic trial will test a culturally-sound family-centred model of care with supported case management by IHWs to improve outcomes for people with complex chronic care needs. This trial is now in the intervention phase.
Australian New Zealand Clinical Trials Registry ACTR12610000812099.
在澳大利亚原住民中,糖尿病和其他常见合并症(高血压、冠心病、肾病和慢性肺病)的患病率和发病率极高。最近采取的一些措施旨在改善原住民社区环境中的预防保健质量,虽然这些措施显然成功地提高了筛查和常规检查的比率,但在适当的护理方面仅取得了适度或较小的改善,例如根据循证指南引入胰岛素和其他扩大药物治疗方案,以及支持降低风险因素。需要制定一项新战略,通过具有适当系统支持的社区护理协调员,确保在当地提供高质量的综合以家庭为中心的护理,具有连续性和文化安全性。
方法/设计:试验设计为开放平行聚类随机对照试验。这项实用试验的目的是测试一种卫生服务提供模式的有效性,该模式有助于在北昆士兰农村和偏远地区的原住民初级保健服务中进行基于社区的强化慢性疾病管理,与常规护理相比。参与者是年龄在 18-65 岁之间、血糖控制不佳(HbA1c>=8.5)且至少患有一种其他慢性疾病的原住民成年人。干预措施是雇佣一名原住民健康工作者对最多 30 名参与者的护理进行病例管理。原住民健康工作者最初接受密集的临床培训,并在整个研究过程中接受培训,以确保他们有能力协调慢性病患者的护理。原住民健康工作者在当地初级保健(PHC)团队和原住民临床支持团队的支持下,将管理护理,包括根据最佳实践标准协调多学科团队护理的机会。在参与者登记后,通过简单随机化对群组进行分组,分配到干预组和对照组。对照组的参与者将接受常规护理,并将候补接受根据数据分析修订的干预模型。主要结局是在 18 个月时测量的 HbA1c 降低。将监测实施一致性,并进行定性调查(待定方法),旨在确定影响慢性病原住民健康结果的模型要素。
这项实用试验将测试一种具有文化意义的以家庭为中心的护理模式,通过 IHW 提供支持性病例管理,以改善有复杂慢性护理需求人群的结果。这项试验现在处于干预阶段。
澳大利亚和新西兰临床试验注册中心 ACTR12610000812099。