Medical Service, Durham Veterans Affairs Medical Center, Durham, North Carolina, USA.
J Thorac Oncol. 2013 Jan;8(1):102-8. doi: 10.1097/JTO.0b013e31827628e1.
We sought to determine the efficacy of using both irinotecan- and etoposide-containing regimens sequentially for patients with untreated limited-stage small-cell lung cancer.
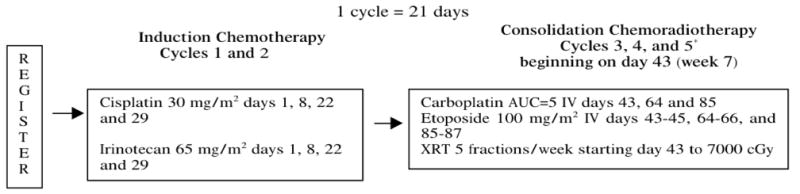
Patients with untreated, measurable, limited-stage small-cell lung cancer with performance status 0 to 2, and adequate organ function were eligible. Treatment consisted of induction with cisplatin 30 mg/m and irinotecan 65 mg/m intravenously on day 1 and 8, every 21 days for two cycles. Beginning day 43, daily chest irradiation to 70 Gy was administered concurrently with carboplatin area under curve 5 on day 1, and etoposide 100 mg/m on days 1 to 3, every 21 days for three cycles. The primary objective was to differentiate between 45% and 60% 2-year survival.
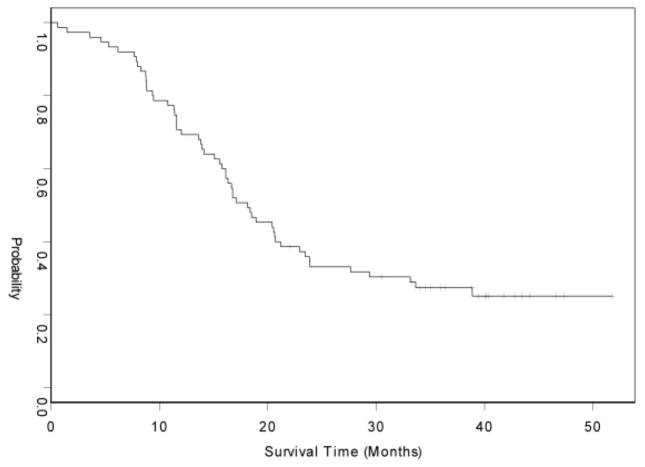
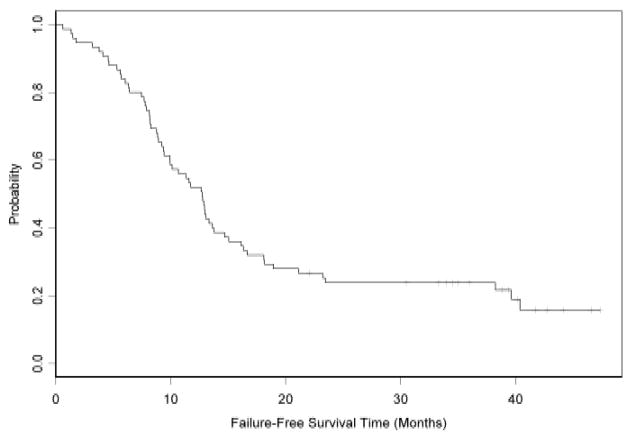
Two induction cycles were delivered to 72 of 75 eligible patients (96%) and all planned treatment was delivered to 59 patients (79%). Cisplatin and irinotecan induction chemotherapy resulted in complete responses in 7% and partial responses in 64% (response rate 71%, 95% confidence interval [CI], 59%-81%). The best response to all therapy included 88% complete or partial responses (95% CI, 78%-94%). With median follow-up of 57 months, the median progression-free survival and overall survival are 12.6 (95% CI, 9.4-14.7) and 18.1 months (15.8-22.9), respectively. The 1- and 2-year survival was 69% and 31%, respectively. Frequent (>20%) grade 3 and 4 toxicities were neutropenia in 84%, hemoglobin in 36%, platelets in 51%, esophagitis in 22%, and dehydration in 24%. There were no fatal toxicities.
This treatment regimen of irinotecan-cisplatin induction chemotherapy followed by 70 Gy concurrent radiation and etoposide-carboplatin had tolerable toxicity but did not meet the preplanned 2-year survival target for further development.
我们旨在确定对于未经治疗的局限期小细胞肺癌患者,序贯使用含伊立替康和依托泊苷方案的疗效。
符合条件的患者为未经治疗、可测量的局限期小细胞肺癌,表现状态为 0-2 级,且器官功能充足。治疗包括顺铂 30 mg/m2 和伊立替康 65 mg/m2 静脉注射,第 1 天和第 8 天,每 21 天为一个周期,共两个周期。从第 43 天开始,每天给予胸部照射至 70 Gy,同时给予卡铂 AUC 5 于第 1 天,依托泊苷 100 mg/m2 于第 1 天至第 3 天,每 21 天为一个周期,共三个周期。主要目标是将 2 年生存率区分在 45%至 60%之间。
75 名符合条件的患者中有 72 名(96%)接受了两个诱导周期的治疗,所有计划的治疗均在 59 名患者(79%)中完成。顺铂和伊立替康诱导化疗的完全缓解率为 7%,部分缓解率为 64%(缓解率为 71%,95%置信区间[CI]为 59%-81%)。所有治疗的最佳反应包括 88%的完全或部分缓解(95%CI,78%-94%)。中位随访 57 个月后,中位无进展生存期和总生存期分别为 12.6 个月(95%CI,9.4-14.7)和 18.1 个月(15.8-22.9)。1 年和 2 年生存率分别为 69%和 31%。>20%的常见 3 级和 4 级毒性为中性粒细胞减少症(84%)、贫血(36%)、血小板减少症(51%)、食管炎(22%)和脱水(24%)。没有致命毒性。
伊立替康-顺铂诱导化疗后再给予 70 Gy 同期放疗和依托泊苷-卡铂的这种治疗方案毒性可耐受,但未达到进一步开发的预定 2 年生存率目标。