Department of Internal Medicine, Division of Cardiology, University of Texas Southwestern Medical Center, Dallas, Texas 75390, USA.
J Am Coll Cardiol. 2013 Jan 15;61(2):187-95. doi: 10.1016/j.jacc.2012.10.012. Epub 2012 Dec 5.
The goal of this study was to determine if biomarkers of subclinical myocardial injury and hemodynamic stress identify asymptomatic individuals with left ventricular hypertrophy (LVH) at higher risk for heart failure (HF) and death.
The interaction between LVH, low but detectable cardiac troponin T (cTnT), and elevated N-terminal pro-B-type natriuretic peptide (NT-proBNP) on cardiovascular (CV) outcomes in the general population is unknown.
Participants in the Dallas Heart Study without clinical HF, LV dysfunction, or chronic kidney disease underwent measurement of LV mass by magnetic resonance imaging (MRI), cTnT by highly sensitive assay, and NT-proBNP analysis (n = 2,413). Subjects were stratified according to LVH and by detectable cTnT (≥3 pg/ml) and increased NT-proBNP (>75th age- and sex-specific percentile) levels. For each analysis, participants were categorized into groups based on the presence (+) or absence (-) of LVH and biomarker levels above (+) or below (-) the predefined threshold.
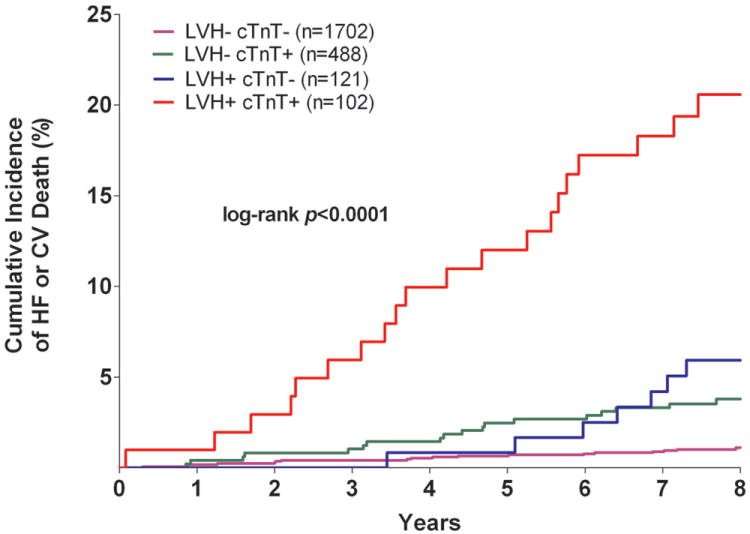
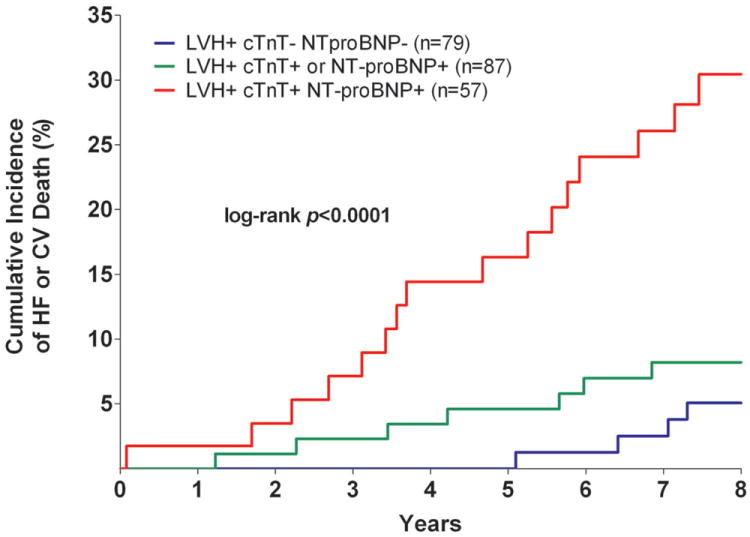
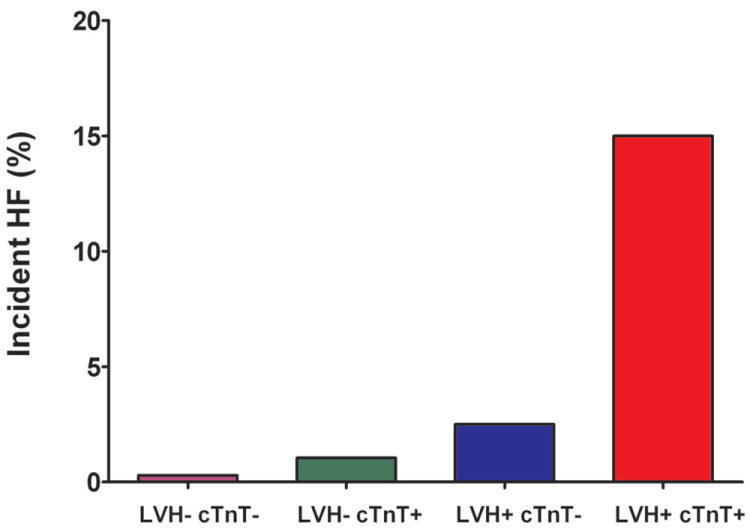
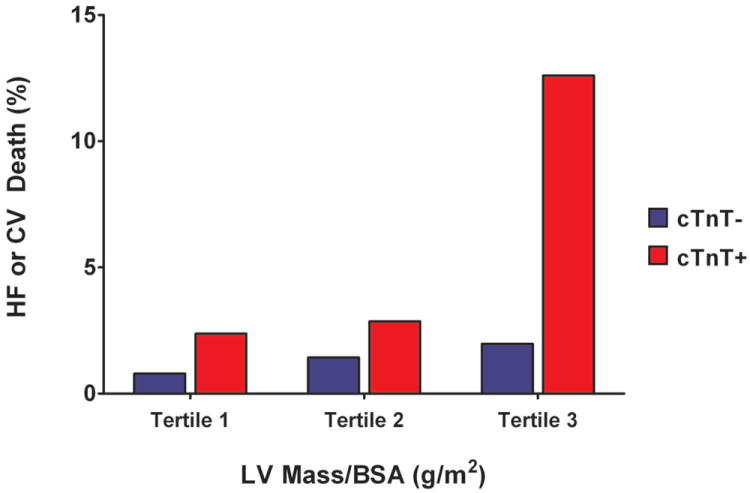
Nine percent of participants were LVH+, 25% cTnT+, and 24% NT-proBNP+. Those LVH+ and cTnT+ and/or NT-proBNP+ (n = 144) were older and more likely to be male, with a greater risk factor burden and more severe LVH compared with those who were LVH+ biomarker- (p < 0.01 for each). The cumulative incidence of HF or CV death over 8 years among LVH+ cTnT+ was 21% versus 1% (LVH- cTnT-), 4% (LVH- cTnT+), and 6% (LVH+ cTnT-) (p < 0.0001). The interactions between LVH and cTnT (p(interaction) = 0.0005) and LVH and NT-proBNP (p(interaction) = 0.014) were highly significant. Individuals who were LVH+ and either cTnT+ or NT-proBNP+ remained at >4-fold higher risk for HF or CV death after multivariable adjustment for CV risk factors, renal function, and LV mass compared with those who were LVH- biomarker-.
Minimal elevations in biomarkers of subclinical cardiac injury and hemodynamic stress modify the association of LVH with adverse outcomes, identifying a malignant subphenotype of LVH with high risk for progression to HF and CV death.
本研究旨在确定亚临床心肌损伤和血流动力学应激的生物标志物是否可识别左心室肥厚(LVH)风险较高的无症状个体,这些个体更容易发生心力衰竭(HF)和死亡。
在普通人群中,LVH 与低但可检测到的心脏肌钙蛋白 T(cTnT)和升高的 N 末端 pro-B 型利钠肽(NT-proBNP)之间的相互作用与心血管(CV)结局之间的相互作用尚不清楚。
达拉斯心脏研究中的参与者无临床 HF、LV 功能障碍或慢性肾脏病,通过磁共振成像(MRI)测量 LV 质量,通过高敏检测分析 cTnT,分析 NT-proBNP(n = 2,413)。根据 LVH 和可检测到的 cTnT(≥3pg/ml)和升高的 NT-proBNP(>75 岁和性别特异性百分位数)水平对受试者进行分层。对于每个分析,根据是否存在(+)或不存在(-)LVH 和生物标志物水平高于(+)或低于(-)预定义阈值,将参与者分为不同组。
9%的参与者为 LVH+,25%为 cTnT+,24%为 NT-proBNP+。与 LVH 标志物-(p < 0.01)相比,LVH+和 cTnT+和/或 NT-proBNP+(n = 144)年龄更大,更可能为男性,危险因素负担更大,LVH 更严重。8 年内 HF 或 CV 死亡的累积发生率在 LVH+ cTnT+中为 21%,而在 LVH- cTnT-中为 1%(LVH- cTnT+)、4%(LVH- cTnT+)和 6%(LVH+ cTnT-)(p < 0.0001)。LVH 与 cTnT 之间的相互作用(p(交互)= 0.0005)和 LVH 与 NT-proBNP 之间的相互作用(p(交互)= 0.014)具有高度显著性。与 LVH-生物标志物-相比,经 CV 危险因素、肾功能和 LV 质量的多变量调整后,LVH 且 cTnT 或 NT-proBNP 升高的个体 HF 或 CV 死亡的风险仍高出 4 倍以上。
亚临床心肌损伤和血流动力学应激的生物标志物的轻微升高改变了 LVH 与不良结局之间的关联,确定了 LVH 与高风险 HF 和 CV 死亡进展相关的恶性亚表型。