The Center for Health Research, Kaiser Permanente Northwest, Portland, OR 97227-1110, USA.
Med Care. 2013 Apr;51(4):324-9. doi: 10.1097/MLR.0b013e3182731277.
Little is known about the medical care resources devoted to diagnosing and treating cancer-related symptoms before a definitive cancer diagnosis. Previous research using SEER-Medicare data to measure incremental costs and utilization associated with cancer started with the date of diagnosis. We hypothesized that health care use increases before diagnosis of a new primary cancer.
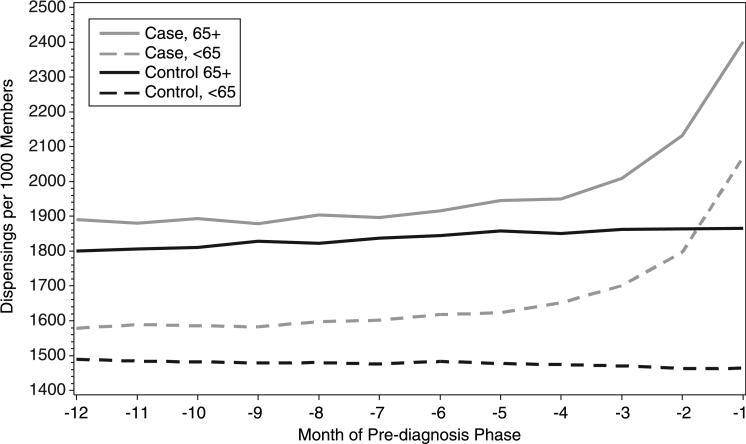
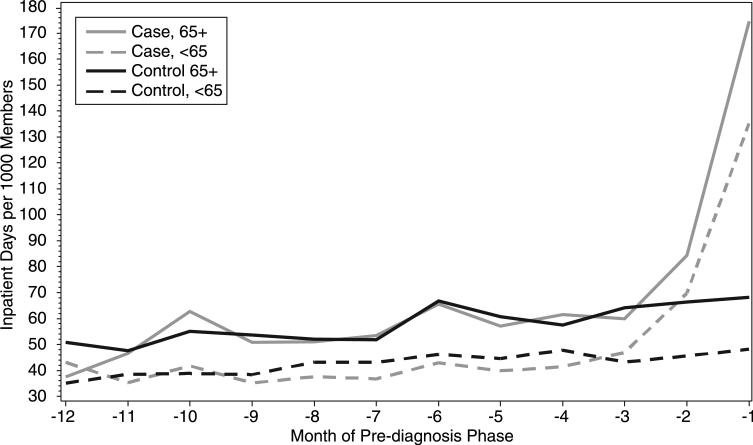
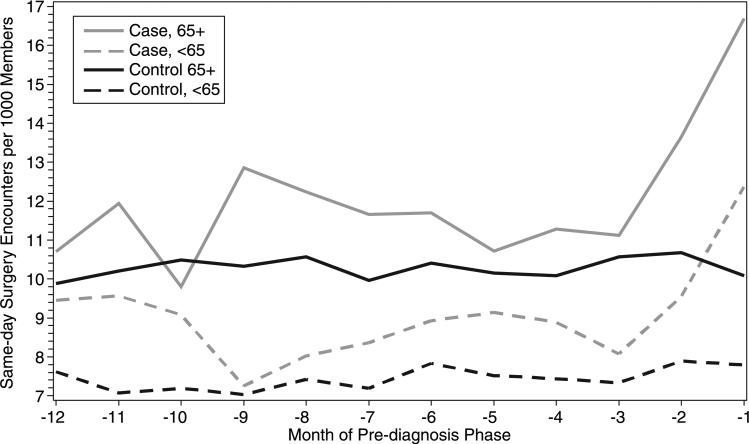
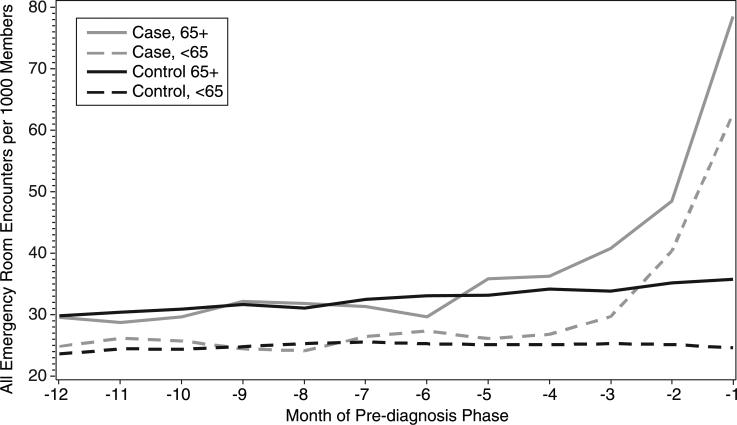
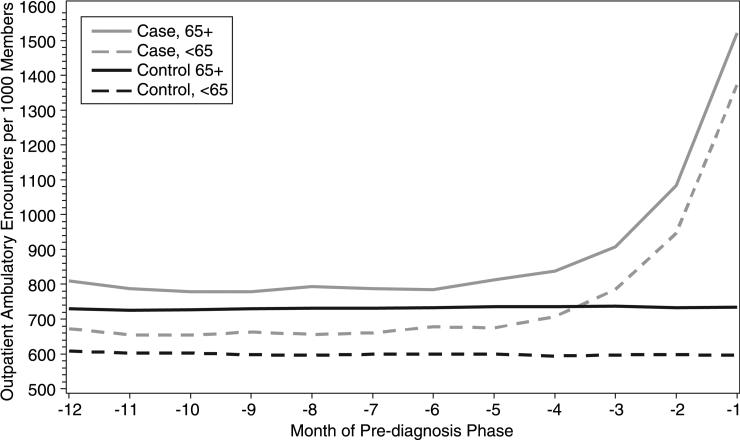
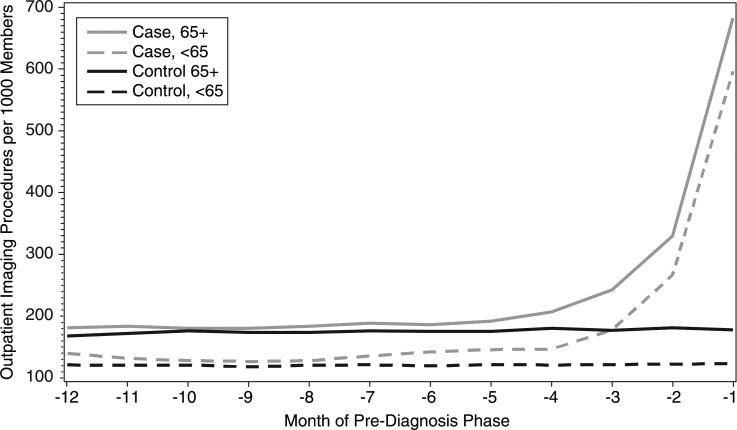
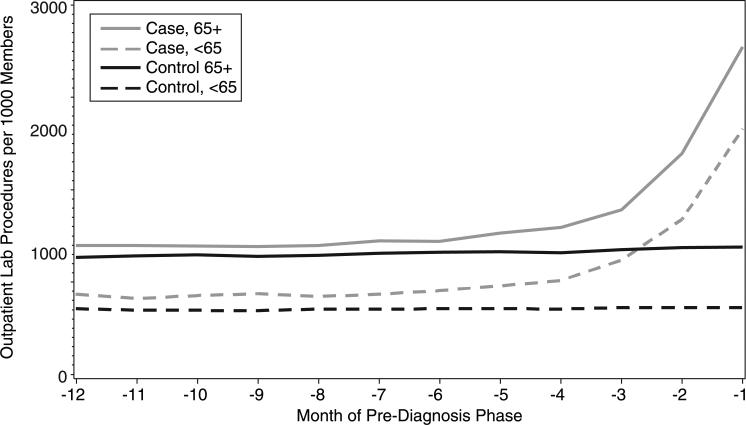
We used a longitudinal case-control design to estimate incremental medical care utilization rates. Cases were 121,293 persons enrolled between January 2000 and December 2008 with ≥1 primary cancers. We selected 522,839 controls randomly from among all health plan members who had no tumor registry evidence of cancer before January 2009, and we frequency matched controls to cancer cases on a 5:1 ratio by age group, sex, and having health plan eligibility in the year of diagnosis of the index cancer case. Utilization data were extracted for all cases and controls for the period 2000 to 2008 from standardized distributed data warehouses. To determine when and the extent to which patterns of medical care use change preceding a cancer diagnosis, we compute hospitalization rates, hospital days, emergency department visits, same-day surgical procedures, ambulatory medical office visits, imaging procedures, laboratory tests, and ambulatory prescription dispensings per 1000 persons per month within integrated delivery systems.
One- to 3-fold increases in monthly utilization rates were observed during the 3 to 5 months before a cancer diagnosis, compared with matched noncancer control groups. This pattern was consistent for both aged and nonaged cancer patients. Aged cancer patients had higher utilization rates than nonaged cancer patients throughout the year before a cancer diagnosis.
The prediagnosis phase is a resource-intensive component of cancer care episodes and should be included in cost of cancer estimates. More research is needed to determine whether reliable prognostic markers can be identified as the start of a cancer episode before a pathology-based diagnosis.
在明确癌症诊断之前,用于诊断和治疗癌症相关症状的医疗资源知之甚少。以前使用 SEER-Medicare 数据来衡量与癌症相关的增量成本和利用情况的研究是从诊断日期开始的。我们假设在新原发性癌症诊断之前,医疗保健的使用会增加。
我们使用纵向病例对照设计来估计增量医疗利用率。病例是 2000 年 1 月至 2008 年 12 月期间至少有 1 种原发性癌症的 121293 人。我们从所有健康计划成员中随机选择了 522839 名对照,他们在 2009 年 1 月之前没有肿瘤登记处的癌症证据,并且我们按年龄组、性别和在指数癌症病例诊断年度的健康计划资格,将对照与癌症病例以 5:1 的比例进行频率匹配。从标准化分布的数据仓库中提取了所有病例和对照在 2000 年至 2008 年期间的利用数据。为了确定在癌症诊断之前医疗保健使用模式何时以及在何种程度上发生变化,我们计算了每 1000 人每月的住院率、住院天数、急诊就诊次数、当日手术次数、门诊医疗办公室就诊次数、影像检查程序、实验室检查和门诊处方配药率。
与匹配的非癌症对照组相比,在癌症诊断前 3 至 5 个月内,每月利用率增加了 1 至 3 倍。这种模式对于老年和非老年癌症患者都是一致的。在癌症诊断前一年中,老年癌症患者的利用率始终高于非老年癌症患者。
诊断前阶段是癌症护理事件的资源密集型组成部分,应包括在癌症成本估计中。需要进一步研究以确定是否可以在基于病理诊断之前确定可靠的预后标志物作为癌症事件的开始。