Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
PLoS One. 2012;7(12):e51225. doi: 10.1371/journal.pone.0051225. Epub 2012 Dec 4.
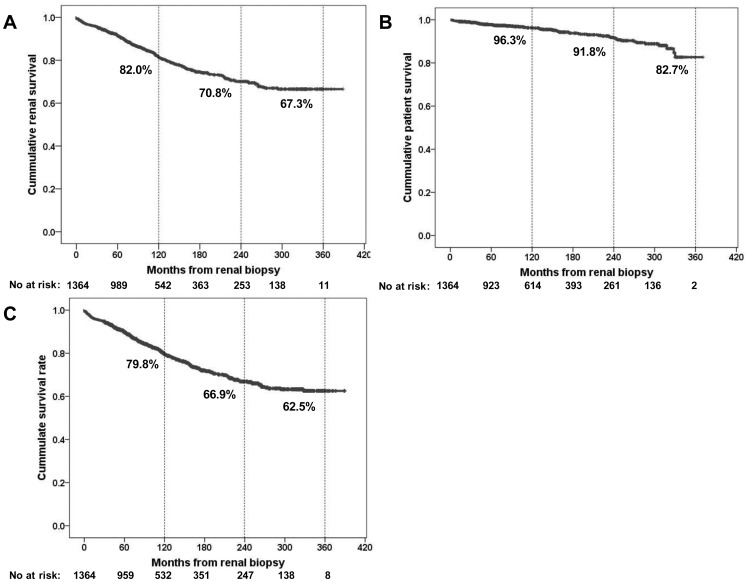
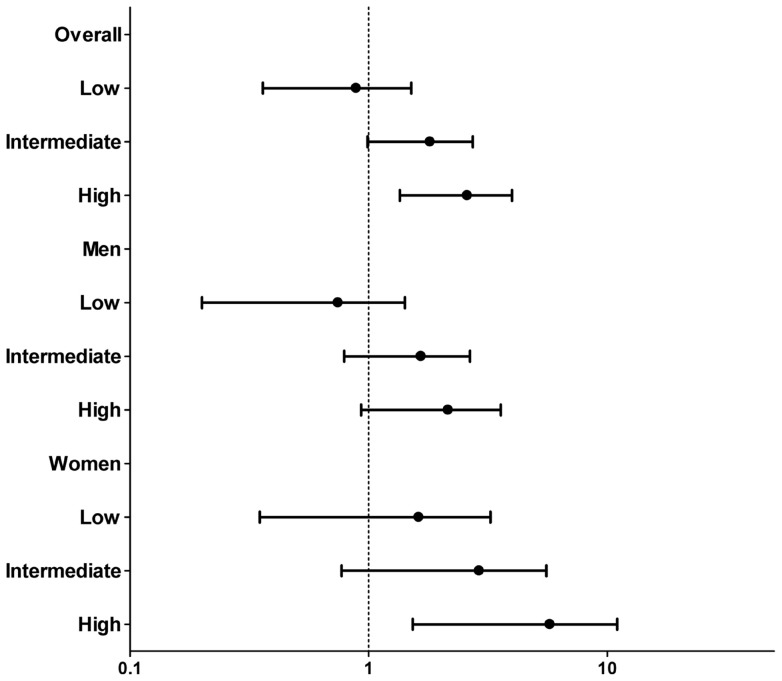
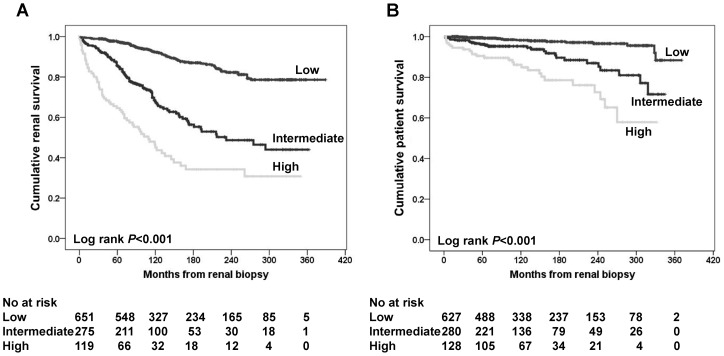
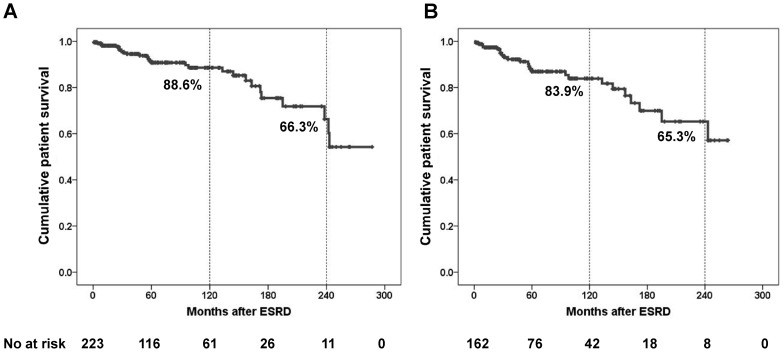
Research on the prognosis of IgA nephropathy (IgAN) has focused on renal survival, with little information being available on patient survival. Hence, this investigation aimed to explore long-term patient outcome in IgAN patients. Clinical and pathological characteristics at the time of renal biopsy were reviewed in 1,364 IgAN patients from 1979 to 2008. The outcomes were patient death and end stage renal disease (ESRD) progression. Overall, 71 deaths (5.3%) and 277 cases of ESRD (20.6%) occurred during 13,916 person-years. Ten-, 20-, and 30-year patient survival rates were 96.3%, 91.8%, and 82.7%, respectively. More than 50% patient deaths occurred without ESRD progression. Overall mortality was elevated by 43% from an age/sex-matched general population (GP) (standardized mortality ratio [SMR], 1.43; 95% confidence interval [CI], 1.04-1.92). Men had comparable mortality to GP (SMR, 1.22; 95% CI, 0.82-1.75), but, in women, the mortality rate was double (SMR, 2.17; 95% CI, 1.21-3.57). Patients with renal risk factors such as initial renal dysfunction (estimated glomerular filgration rate <60 ml/min per 1.73 m(2); SMR, 1.70; 95% CI, 1.13-2.46), systolic blood pressure ≥ 140 mmHg (SMR, 1.88; 95% CI, 1.19-2.82) or proteinuria ≥ 1 g/day (SMR, 1.66; 95% CI, 1.16-2.29) had an elevated mortality rate. Patients with preserved renal function, normotension, and proteinuria <1 g/day, however, had a similar mortality rate to GP. When risk stratification was performed by counting the number of major risk factors present at diagnosis, low-risk IgAN patients had a mortality rate equal to that of GP, whereas high-risk patients had a mortality rate higher than that of GP. This investigation demonstrated that overall mortality in IgAN patients was higher than that of GP. Women and patients with renal risk factors had a higher mortality than that of GP, Therefore, strategies optimized to alleviate major renal risk factors are warranted to reduce patient mortality.
IgA 肾病(IgAN)的预后研究主要集中在肾脏生存方面,而患者生存方面的信息却很少。因此,本研究旨在探讨 IgAN 患者的长期预后。对 1979 年至 2008 年间 1364 例 IgAN 患者的肾活检时的临床和病理特征进行了回顾性分析。结果为患者死亡和终末期肾病(ESRD)进展。在 13916 人年的随访中,共有 71 例(5.3%)死亡和 277 例 ESRD(20.6%)。10、20 和 30 年的患者生存率分别为 96.3%、91.8%和 82.7%。超过 50%的患者死亡发生在没有 ESRD 进展的情况下。总体死亡率比年龄和性别匹配的一般人群(GP)高 43%(标准化死亡率比[SMR],1.43;95%置信区间[CI],1.04-1.92)。男性的死亡率与 GP 相当(SMR,1.22;95% CI,0.82-1.75),但女性的死亡率则是男性的两倍(SMR,2.17;95% CI,1.21-3.57)。有肾脏危险因素的患者,如初始肾功能障碍(估计肾小球滤过率<60 ml/min/1.73 m(2);SMR,1.70;95% CI,1.13-2.46)、收缩压≥140 mmHg(SMR,1.88;95% CI,1.19-2.82)或蛋白尿≥1 g/天(SMR,1.66;95% CI,1.16-2.29),死亡率较高。然而,具有正常肾功能、血压和蛋白尿<1 g/天的患者的死亡率与 GP 相似。当根据诊断时存在的主要危险因素数量进行风险分层时,低危 IgAN 患者的死亡率与 GP 相同,而高危患者的死亡率高于 GP。本研究表明,IgAN 患者的总体死亡率高于 GP。女性和有肾脏危险因素的患者的死亡率高于 GP,因此,需要采取优化策略来减轻主要肾脏危险因素,以降低患者死亡率。