Department of Pediatric, APHP, Hôpital Antoine Béclère, Service de Pédiatrie, 157 rue de la porte de Trivaux, 92141 Clamart Cedex, France.
Exp Hematol Oncol. 2012 Dec 10;1(1):39. doi: 10.1186/2162-3619-1-39.
Clofarabine alone or in combination with cyclophosphamide and etoposide has shown a good efficacy and a tolerable toxicity profile in previous studies of children with relapsed or refractory leukaemia. This report describes a retrospective study of 38 French patients who received clofarabine as a monotherapy or in combination for relapsed or refractory acute lymphoblastic leukaemia (ALL) outside of clinical trials after marketing authorization.
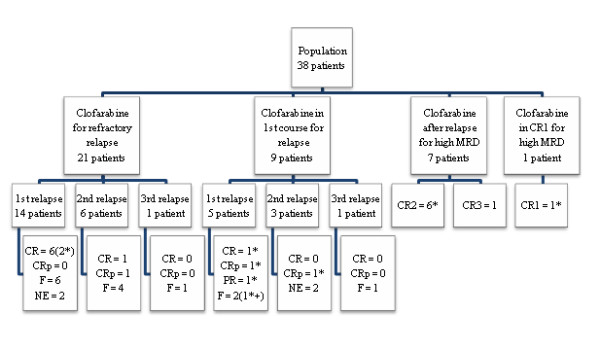
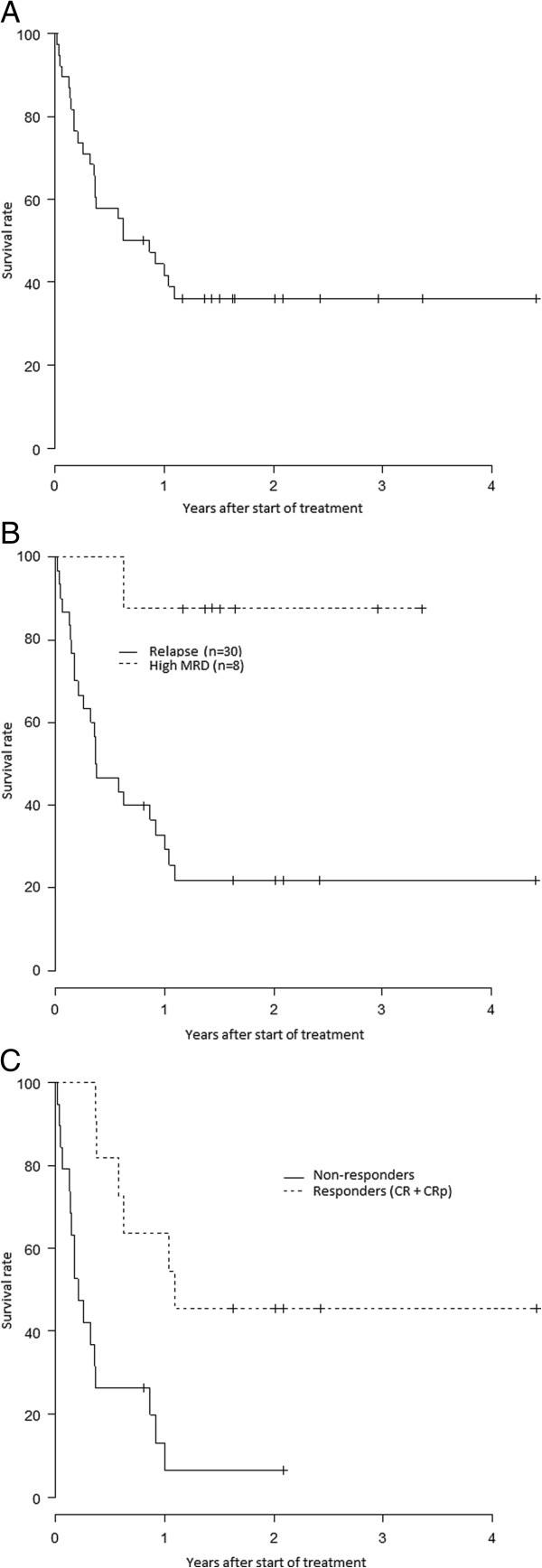
We retrospectively analysed data for 38 patients, up to 21 years old, attending 17 French centres. Thirty patients received clofarabine alone or in combination for a bone marrow relapse of acute lymphoblastic leukaemia (ALL) or refractory disease and eight patients for a high level of minimal residual disease (MRD). Survival and response durations were estimated by the Kaplan-Meier method.
For the 30 patients who received clofarabine for a bone marrow relapse of ALL (number of relapse, 1-3; median, 1), the overall remission rate (ORR) was 37%: eight complete remission (CR) and three complete remission without platelet recovery (CRp). Ten of the 11 responding patients subsequently underwent haematopoietic stem cell transplantation (HSCT).Only four of the eight patients who received clofarabine while in remission for a high level of MRD, showed a moderate improvement of MRD. Seven of these eight patients received HSCT and six of them were alive at the end of the study. One other patient was alive without receiving HSCT.However, clofarabine treatment was associated with a high risk of infection and hepatotoxicity. Febrile neutropenia grade ≥ 3 was reported in 79% of patients and documented infections grade ≥ 3 occurred in nine patients (24%). Hepatotoxicity grade 3 was reported in nine patients (24%). We observed four deaths related to treatment.
In our experience, the efficacy of clofarabine is poorer than previously reported. Its toxicity is high and can be life threatening. Prospective studies on clofarabine used during earlier phases of the disease may help to define how best this new drug can be exploited for childhood and adolescent ALL.
在先前的研究中,单独使用氯法拉滨或与环磷酰胺和依托泊苷联合使用,在复发或难治性白血病患儿中显示出良好的疗效和可耐受的毒性特征。本报告描述了一项回顾性研究,38 名法国患者在获得氯法拉滨上市许可后,在临床试验之外,使用该药单药或联合方案治疗复发或难治性急性淋巴细胞白血病(ALL)。
我们对 17 家法国中心的 38 名年龄在 21 岁以下的患者进行了回顾性数据分析。30 名患者接受氯法拉滨单药或联合方案治疗骨髓复发的 ALL(复发次数为 1-3,中位数为 1)或难治性疾病,8 名患者接受氯法拉滨治疗高水平微小残留病(MRD)。采用 Kaplan-Meier 法估计生存和缓解持续时间。
30 名接受氯法拉滨治疗骨髓复发 ALL 的患者(复发次数为 1-3,中位数为 1),总体缓解率(ORR)为 37%:8 例完全缓解(CR),3 例血小板未恢复的完全缓解(CRp)。11 例缓解患者中有 10 例随后接受了造血干细胞移植(HSCT)。仅 8 例接受氯法拉滨治疗以缓解高水平 MRD 的患者中,4 例 MRD 中度改善。这 8 例患者中有 7 例接受了 HSCT,6 例在研究结束时仍存活。另 1 例患者未接受 HSCT 但仍存活。然而,氯法拉滨治疗与感染和肝毒性的风险较高相关。79%的患者出现发热性中性粒细胞减少症≥3 级,9 例患者出现≥3 级的有记录的感染(24%)。9 例患者(24%)出现 3 级肝毒性。我们观察到 4 例与治疗相关的死亡。
根据我们的经验,氯法拉滨的疗效不如先前报道的那样好。其毒性较高,可能危及生命。关于氯法拉滨在疾病早期阶段使用的前瞻性研究可能有助于确定如何最好地利用这种新药治疗儿童和青少年 ALL。