Hanekom Susan D, Louw Quinette, Coetzee Andre
Crit Care. 2012 Dec 11;16(6):R230. doi: 10.1186/cc11894.
The physiological basis of physiotherapeutic interventions used in intensive care has been established. We must determine the optimal service approach that will result in improved patient outcome. The aim of this article is to report on the estimated effect of providing a physiotherapy service consisting of an exclusively allocated physiotherapist providing evidence-based/protocol care, compared with usual care on patient outcomes.
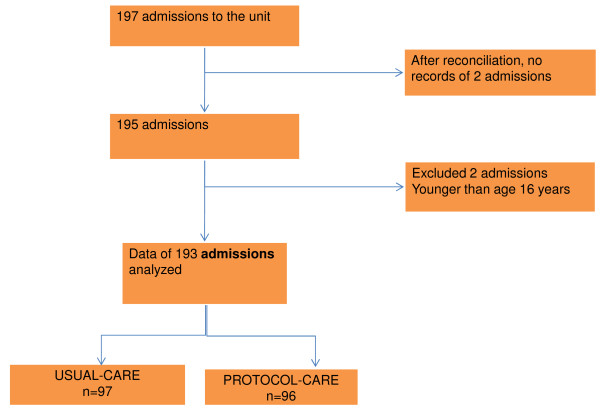
An exploratory, controlled, pragmatic, sequential-time-block clinical trial was conducted in the surgical unit of a tertiary hospital in South Africa. Protocol care (3 weeks) and usual care (3 weeks) was provided consecutively for two 6-week intervention periods. Each intervention period was followed by a washout period. The physiotherapy care provided was based on the unit admission date. Data were analyzed with Statistica in consultation with a statistician. Where indicated, relative risks with 95% confidence intervals (CIs) are reported. Significant differences between groups or across time are reported at the alpha level of 0.05. All reported P values are two-sided.
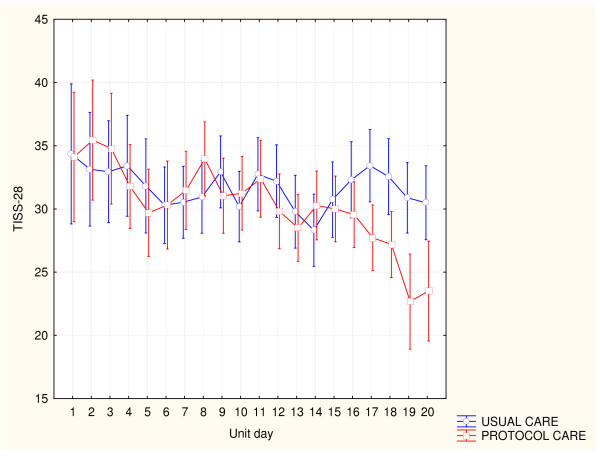
Data of 193 admissions were analyzed. No difference was noted between the two patient groups at baseline. Patients admitted to the unit during protocol care were less likely to be intubated after unit admission (RR, 0.16; 95% CI, 0.07 to 0.71; RRR, 0.84; NNT, 5.02; P = 0.005) or to fail an extubation (RR, 0.23; 95% CI, 0.05 to 0.98; RRR, 0.77; NNT, 6.95; P = 0.04). The mean difference in the cumulative daily unit TISS-28 score during the two intervention periods was 1.99 (95% CI, 0.65 to 3.35) TISS-28 units (P = 0.04). Protocol-care patients were discharged from the hospital 4 days earlier than usual-care patients (P = 0.05). A tendency noted for more patients to reach independence in the transfers (P = 0.07) and mobility (P = 0.09) categories of the Barthel Index.
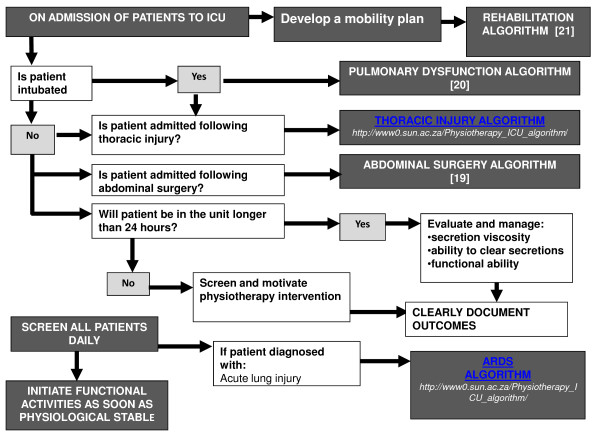
A physiotherapy service approach that includes an exclusively allocated physiotherapist providing evidence-based/protocol care that addresses pulmonary dysfunction and promotes early mobility improves patient outcome. This could be a more cost-effective service approach to care than is usual care. This information can now be considered by administrators in the management of scarce physiotherapy resources and by researchers in the planning of a multicenter randomized controlled trial.
PACTR201206000389290.
重症监护中使用的物理治疗干预措施的生理基础已得到确立。我们必须确定能改善患者预后的最佳服务方式。本文旨在报告由专门分配的物理治疗师提供循证/规范护理的物理治疗服务与常规护理相比对患者预后的估计效果。
在南非一家三级医院的外科病房进行了一项探索性、对照、务实、序贯时间块临床试验。在两个为期6周的干预期内,依次提供规范护理(3周)和常规护理(3周)。每个干预期后有一个洗脱期。所提供的物理治疗护理基于病房入院日期。与统计学家协商后使用Statistica软件分析数据。在有指示的情况下,报告95%置信区间(CI)的相对风险。组间或不同时间的显著差异在α水平为0.05时报告。所有报告的P值均为双侧。
分析了193例入院患者的数据。两组患者在基线时无差异。在规范护理期间入住病房的患者入院后插管的可能性较小(相对风险,0.16;95%CI,0.07至0.71;相对风险降低率,0.84;需治疗人数,5.02;P = 0.005)或拔管失败的可能性较小(相对风险,0.23;95%CI,0.05至0.98;相对风险降低率,0.77;需治疗人数,6.95;P = 0.04)。两个干预期内每日累计单位TISS - 28评分的平均差异为1.99(95%CI,0.65至3.35)个TISS - 28单位(P = 0.04)。接受规范护理的患者比接受常规护理的患者提前4天出院(P = 0.05)。在Barthel指数的转移(P = 0.07)和活动能力(P = 0.09)类别中,有更多患者达到独立的趋势。
一种物理治疗服务方式,包括专门分配的物理治疗师提供针对肺功能障碍并促进早期活动的循证/规范护理,可改善患者预后。这可能是一种比常规护理更具成本效益的护理服务方式。医院管理人员在管理稀缺的物理治疗资源时以及研究人员在规划多中心随机对照试验时现在可以考虑这些信息。
PACTR201206000389290