Department of Oncological Surgery, Medical University of Gdańsk, Gdańsk, Poland.
Arch Gynecol Obstet. 2013 Jun;287(6):1211-8. doi: 10.1007/s00404-012-2683-x. Epub 2012 Dec 22.
In 2009, International Federation of Gynecology and Obstetrics (FIGO) modified staging of vulvar cancer-the prognostic significance of the new classification relative to the prior system as well as to the commonly recognized prognostic factors has not been assessed. The aim of this study was to test prognostic ability of 2009 staging in a cohort of uniformly treated and staged cases with long-term follow-up.
Pathologic characteristics were obtained by blind review of the original tissue samples. 76 patients who qualified for surgery on the basis of the same criteria, with full clinical history, were included in the study. The histological analyses were performed on 76 and 35 paraffin-embedded tissue samples from primary tumors and lymph nodes, respectively. Survival analyses included the Kaplan-Meier method, log-rank test and Cox proportional hazards model.
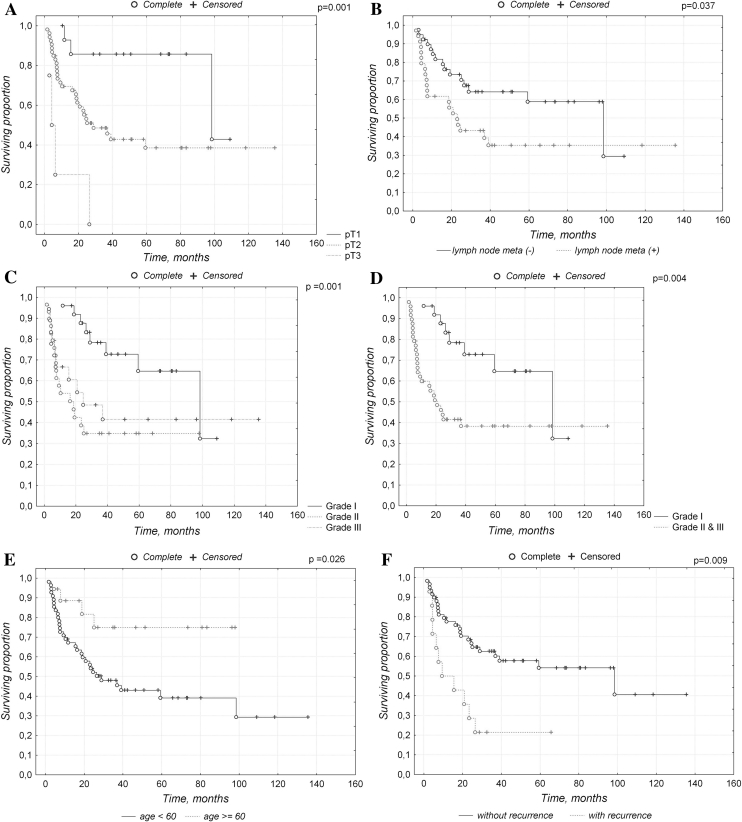
Univariate analysis has demonstrated that age (p = 0.0170), lymph node metastasis (p = 0.0393), tumor grade (p = 0.0086) and FIGO1994 stage (p = 0.001) were the significant prognostic factors for overall survival. Multivariate analysis has demonstrated that growing age (HR 2.25, 95 % CI 0.79-3.71, p = 0.0321), tumor grade (G1 vs. G2 and G3) (HR 1-3.11, 95 % CI 1.6-4.62, p = 0.0057) and FIGO1994 stage (HR 1.78, 95 % CI 0.55-3.01, p = 0.0061) are independent prognostic factors with respect to overall survival.
The results indicate the prognostic advantage of the 1994 FIGO staging as it has become an independent prognostic factor in contrast to the new FIGO system. This should be tested in future larger cohort studies. Differentiation grade turned out to be a very valuable independent prognostic factor and should be incorporated as a routine component of the histopathologic reports in vulvar cancer.
2009 年,国际妇产科联合会(FIGO)修改了外阴癌的分期-新分类与先前系统以及公认的预后因素的相关性的预后意义尚未得到评估。本研究的目的是在一组经过长期随访的统一治疗和分期的病例中测试 2009 分期的预后能力。
通过对原始组织样本进行盲法复查获得病理特征。根据相同标准有手术资格且具有完整临床病史的 76 名患者被纳入研究。对 76 例原发性肿瘤和 35 例淋巴结石蜡包埋组织样本进行了组织学分析。生存分析包括 Kaplan-Meier 法、log-rank 检验和 Cox 比例风险模型。
单因素分析表明,年龄(p=0.0170)、淋巴结转移(p=0.0393)、肿瘤分级(p=0.0086)和 FIGO1994 分期(p=0.001)是总生存的显著预后因素。多因素分析表明,年龄增长(HR 2.25,95%CI 0.79-3.71,p=0.0321)、肿瘤分级(G1 与 G2 和 G3)(HR 1-3.11,95%CI 1.6-4.62,p=0.0057)和 FIGO1994 分期(HR 1.78,95%CI 0.55-3.01,p=0.0061)是总生存的独立预后因素。
结果表明 1994 年 FIGO 分期具有预后优势,因为它已成为独立的预后因素,而不是新的 FIGO 系统。这应该在未来更大的队列研究中进行测试。分化程度被证明是一个非常有价值的独立预后因素,应该作为外阴癌组织病理学报告的常规组成部分纳入。