Department of Gynaecological Oncology, Royal Hallamshire Hospital, Sheffield, UK.
BJOG. 2013 Mar;120(4):400-10; discussion 410-1. doi: 10.1111/1471-0528.12096. Epub 2013 Jan 4.
To determine if electrical impedance spectroscopy (EIS) improves the diagnostic accuracy of colposcopy when used as an adjunct.
Prospective, comparative, multi-centre clinical study.
Three colposcopy clinics: two in England and one in Ireland.
Women referred with abnormal cytology.
In phase 1, EIS was assessed against colposcopic impression and histopathology of the biopsies taken. In phase 2, a probability index and cut-off value for the detection of high-grade cervical intraepithelial neoplasia (HG-CIN, i.e. grade CIN2+) was derived to indicate sites for biopsy. EIS data collection and analyses were performed in real time and blinded to the clinician. The phase-2 data were analysed using different cut-off values to assess performance of EIS as an adjunct.
Histologically confirmed HG-CIN (CIN2+).
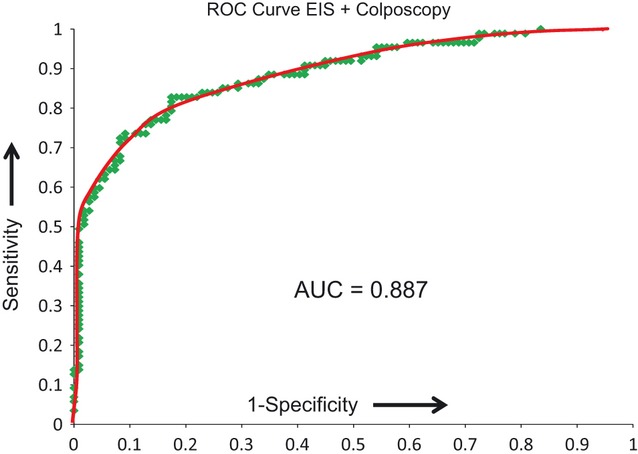
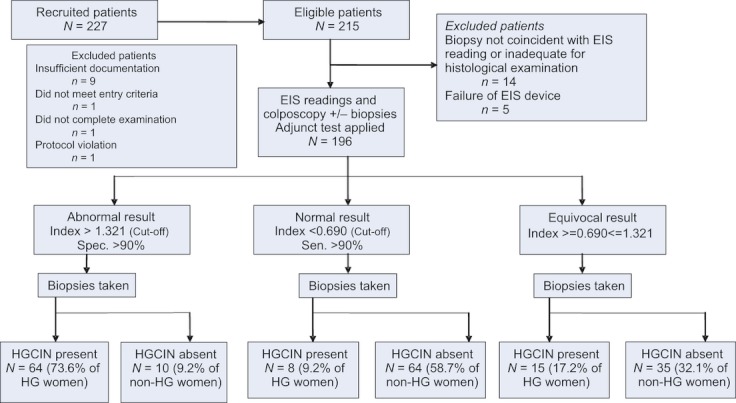
A total of 474 women were recruited: 214 were eligible for analysis in phase 1, and 215 were eligible in phase 2. The average age was 33.2 years (median age 30.3 years, range 20-64 years) and 48.5% (208/429) had high-grade cytology. Using the cut-off from phase 1 the accuracy of colposcopic impression to detect HG-CIN when using EIS as an adjunct at the time of examination improved the positive predictive value (PPV) from 78.1% (95% CI 67.5-86.4) to 91.5%. Specificity was also increased from 83.5% (95% CI 75.2-89.9) to 95.4%, but sensitivity was significantly reduced from 73.6% (95% CI 63.0-82.5) to 62.1%, and the negative predictive value (NPV) was unchanged. The positive likelihood ratio for colposcopic impression alone was 4.46. This increased to 13.5 when EIS was used as an adjunct. The overall accuracy of colposcopy when used with EIS as an adjunct was assessed by varying the cut-off applied to a combined test index. Using a cut-off set to give the same sensitivity as colposcopy in phase 2, EIS increased the PPV to detect HG-CIN from 53.5% (95% CI 45.0-61.8) to 67%, and specificity increased from 38.5% (95% CI 29.4-48.3) to 65.1%. NPV was not significantly increased. Alternatively, applying a cut-off to give the same specificity as colposcopy alone increased EIS sensitivity from 88.5% (95% CI 79.9-94.4) to 96.6%, and NPV from 80.8% (95% CI 67.5-90.4) to 93.3%. PPV was not significantly increased. The receiver operator characteristic (ROC) to detect HG-CIN had an area under the curve (AUC) of 0.887 (95% CI 0.840-0.934).
EIS used as an adjunct to colposcopy improves colposcopic performance. The addition of EIS could lead to more appropriate patient management with lower intervention rates.
确定在阴道镜检查中作为辅助手段使用时,阻抗光谱分析(EIS)是否可以提高诊断准确性。
前瞻性、对比、多中心临床研究。
三家阴道镜诊所:两家在英国,一家在爱尔兰。
细胞学异常转诊的女性。
在第一阶段,EIS 与阴道镜印象和活检的组织病理学进行了评估。在第二阶段,为了检测高级别宫颈上皮内瘤变(HG-CIN,即 CIN2+),得出了一个概率指数和截断值,以指示活检部位。EIS 数据采集和分析实时进行,并对临床医生进行了盲法处理。使用不同的截断值分析了第二阶段的数据,以评估 EIS 作为辅助手段的性能。
组织学证实的 HG-CIN(CIN2+)。
共招募了 474 名女性:214 名符合第一阶段分析标准,215 名符合第二阶段分析标准。平均年龄为 33.2 岁(中位数年龄为 30.3 岁,范围为 20-64 岁),48.5%(208/429)有高级别细胞学。使用第一阶段的截断值,当在检查时将 EIS 作为辅助手段使用时,阴道镜印象检测 HG-CIN 的准确性提高了阳性预测值(PPV),从 78.1%(95%CI 67.5-86.4)提高到 91.5%。特异性也从 83.5%(95%CI 75.2-89.9)提高到 95.4%,但敏感性显著降低,从 73.6%(95%CI 63.0-82.5)降低到 62.1%,阴性预测值(NPV)保持不变。阴道镜印象单独的阳性似然比为 4.46。当 EIS 作为辅助手段使用时,这一数值增加到 13.5。当 EIS 作为辅助手段使用时,阴道镜的总体准确性通过改变应用于联合测试指数的截断值进行评估。使用设定为与第二阶段阴道镜相同敏感性的截断值,EIS 将检测 HG-CIN 的 PPV 从 53.5%(95%CI 45.0-61.8)提高到 67%,特异性从 38.5%(95%CI 29.4-48.3)提高到 65.1%。NPV 没有显著增加。或者,应用一个截断值以获得与阴道镜单独使用相同的特异性,可使 EIS 的敏感性从 88.5%(95%CI 79.9-94.4)提高到 96.6%,NPV 从 80.8%(95%CI 67.5-90.4)提高到 93.3%。PPV 没有显著增加。检测 HG-CIN 的受试者工作特征(ROC)曲线下面积(AUC)为 0.887(95%CI 0.840-0.934)。
EIS 作为阴道镜检查的辅助手段可以提高阴道镜检查的性能。EIS 的加入可以降低干预率,从而实现更合理的患者管理。