Department of Rheumatology, Aarhus University Hospital, Aarhus, Denmark.
PLoS One. 2012;7(12):e53034. doi: 10.1371/journal.pone.0053034. Epub 2012 Dec 27.
Arthritic bone loss in the joints of patients with rheumatoid arthritis is the result of a combination of osteoclastic bone resorption and osteoblastic bone formation. This process is not completely understood, and especially the importance of local inflammation needs further investigation. We evaluated how bone formation and bone resorption are altered in experimental autoimmune arthritis.
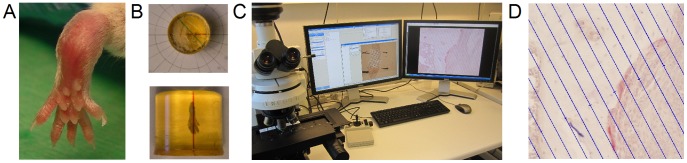
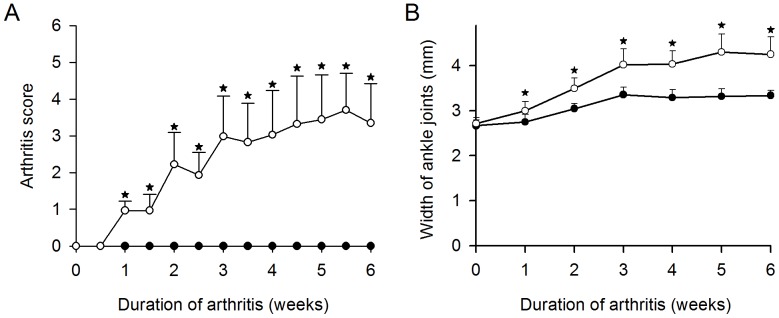
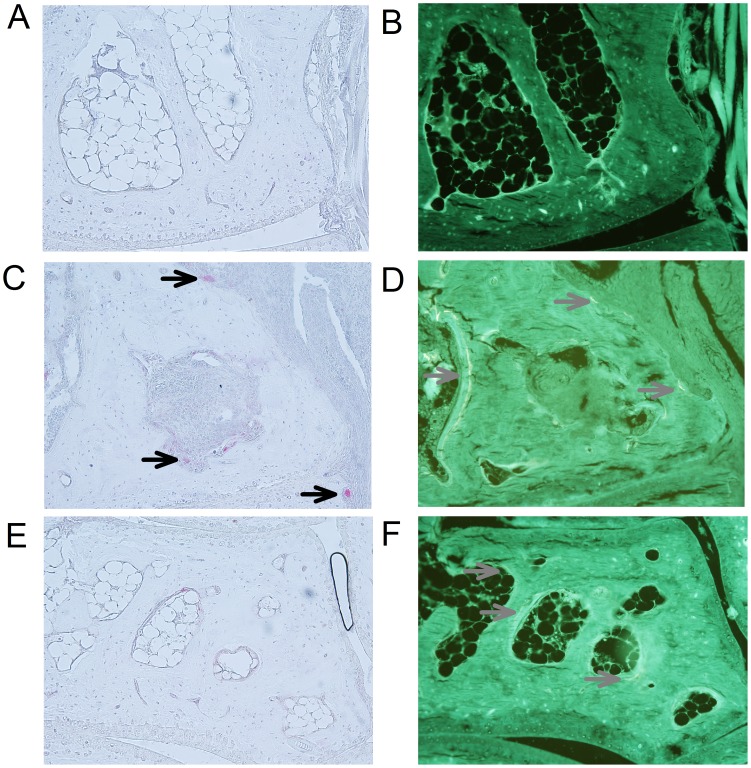
Twenty-one female SKG mice were randomized to either an arthritis group or a control group. Tetracycline was used to identify mineralizing surfaces. After six weeks the right hind paws were embedded undecalcified in methylmethacrylate. The paws were cut exhaustively according to the principles of vertical sectioning and systematic sampling. 3D design-based methods were used to estimate the total number of osteoclasts, mineralizing surfaces, eroded surfaces, and osteoclast-covered bone surfaces. In addition the presence of adjacent inflammation was ascertained.
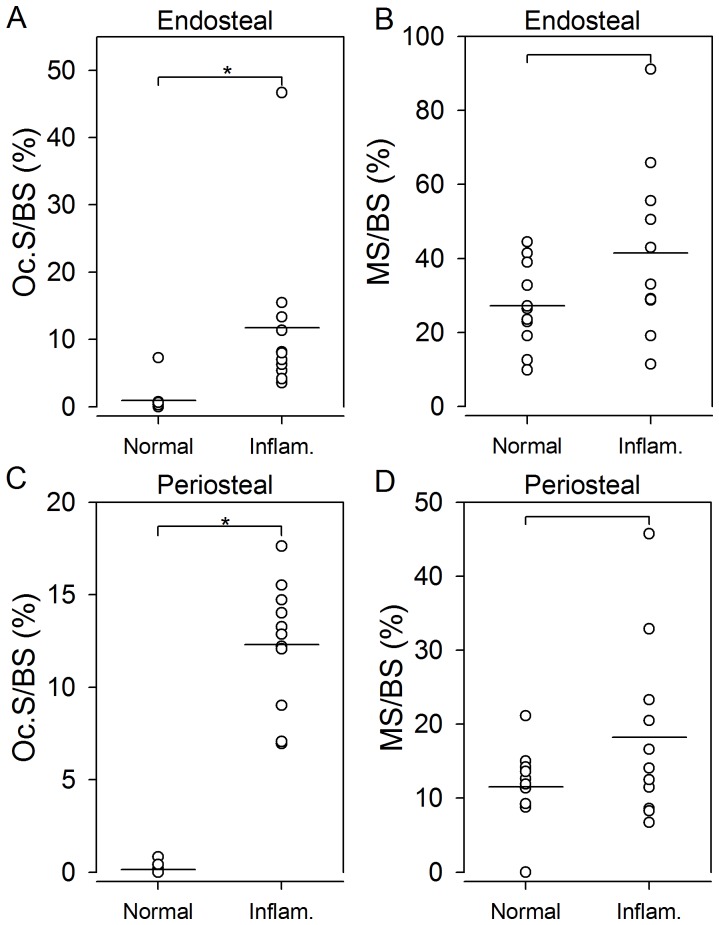
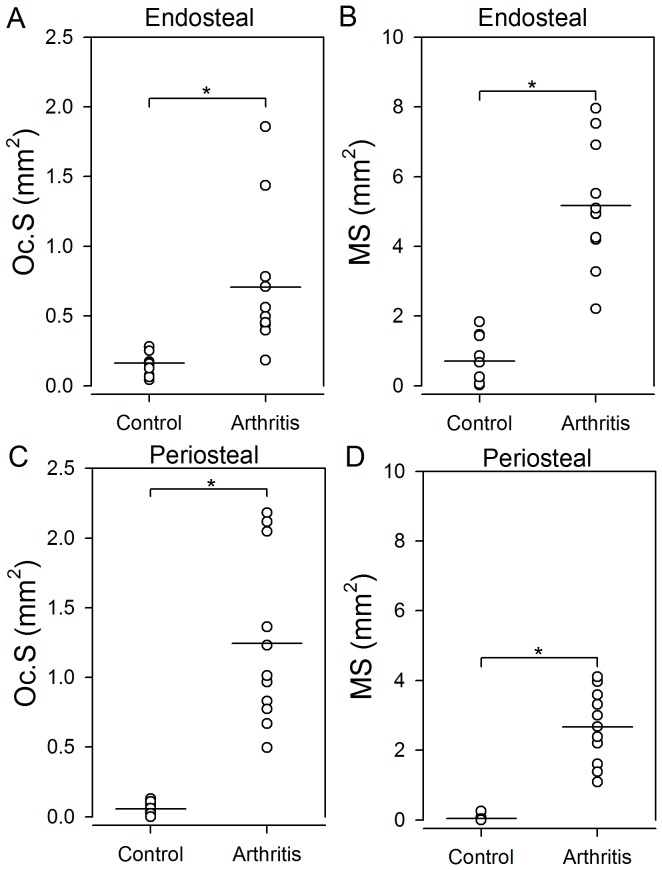
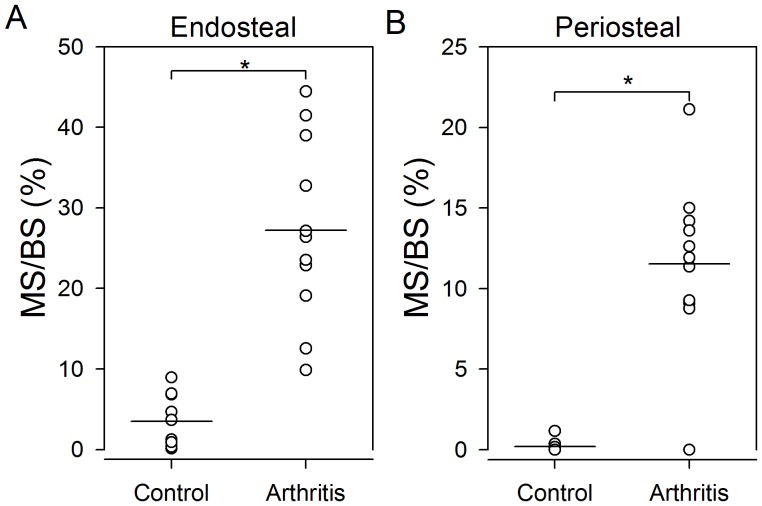
The total number of osteoclasts, mineralizing surfaces, eroded surfaces, and osteoclast covered surfaces were elevated in arthritic paws compared to normal paws. Mineralizing surfaces were elevated adjacent to as well as not adjacent to inflammation in arthritic mice compared to normal mice. In arthritic mice, eroded surfaces and osteoclast covered surfaces were larger on bone surfaces adjacent to inflammation than on bone surfaces without adjacent inflammation. However, we found no difference between mineralizing surfaces at bone surfaces with or without inflammation in arthritic mice.
Inflammation induced an increase in resorptive bone surfaces as well as formative bone surfaces. The bone formative response may be more general, since formative bone surfaces were also increased when not associated with inflammation. Thus, the bone loss may be the result of a substantial local bone resorption, which cannot be compensated by the increased local bone formation. These findings may be valuable for the development of new osteoblast targeting drugs in RA.
类风湿关节炎患者关节中的关节炎性骨丢失是破骨细胞骨吸收和成骨细胞骨形成相结合的结果。这一过程尚未完全被理解,特别是局部炎症的重要性需要进一步研究。我们评估了实验性自身免疫性关节炎中骨形成和骨吸收的变化。
21 只雌性 SKG 小鼠被随机分为关节炎组或对照组。四环素用于识别矿化表面。六周后,将右后爪嵌入甲基丙烯酸甲酯中不脱钙。根据垂直切片和系统取样的原则,将爪子彻底切割。使用基于 3D 设计的方法来估计破骨细胞总数、矿化表面、侵蚀表面和破骨细胞覆盖的骨表面。此外,还确定了相邻炎症的存在。
与正常爪子相比,关节炎爪子中的破骨细胞总数、矿化表面、侵蚀表面和破骨细胞覆盖的表面都升高了。与正常小鼠相比,关节炎小鼠中矿化表面在炎症相邻和不相邻处都升高了。在关节炎小鼠中,与无炎症相邻的骨表面相比,炎症相邻的骨表面上的侵蚀表面和破骨细胞覆盖的表面更大。然而,我们发现在关节炎小鼠中,炎症相邻和无炎症相邻的骨表面上的矿化表面没有差异。
炎症诱导了吸收性骨表面和形成性骨表面的增加。成骨反应可能更为普遍,因为当不与炎症相关时,形成性骨表面也会增加。因此,骨丢失可能是局部骨吸收的结果,这种骨吸收不能被增加的局部骨形成所补偿。这些发现可能对开发治疗类风湿关节炎的新成骨靶向药物有价值。