Oxford University Clinical Research Unit, Hospital for Tropical Diseases, Ho Chi Minh City, Vietnam.
Intensive Care Med. 2013 Apr;39(4):661-71. doi: 10.1007/s00134-012-2771-1. Epub 2013 Jan 10.
To quantify the effects of barrier precautions and antibiotic mixing on prevalence and acquisition of five drug-resistant microorganisms within a single tetanus intensive care unit at a tertiary referral hospital in Ho Chi Minh City, Vietnam.
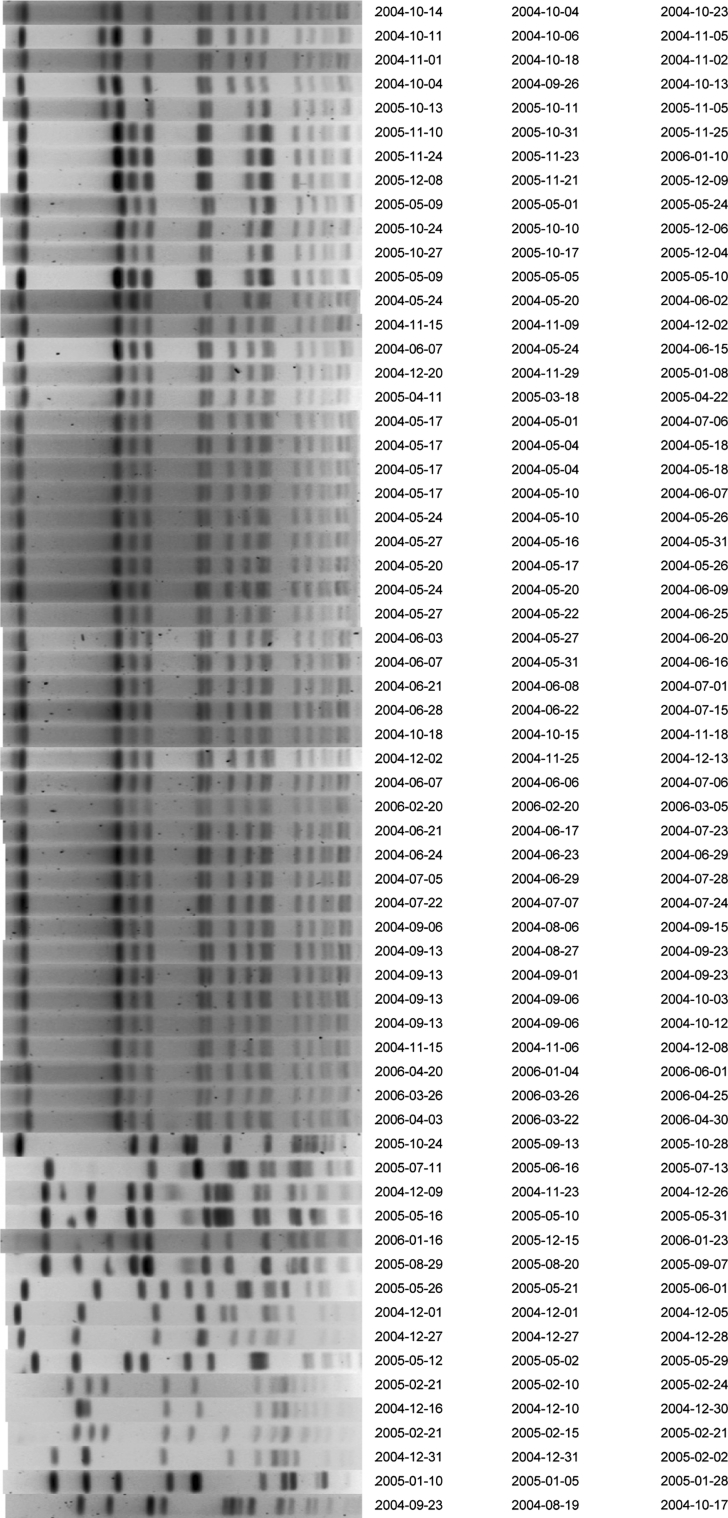
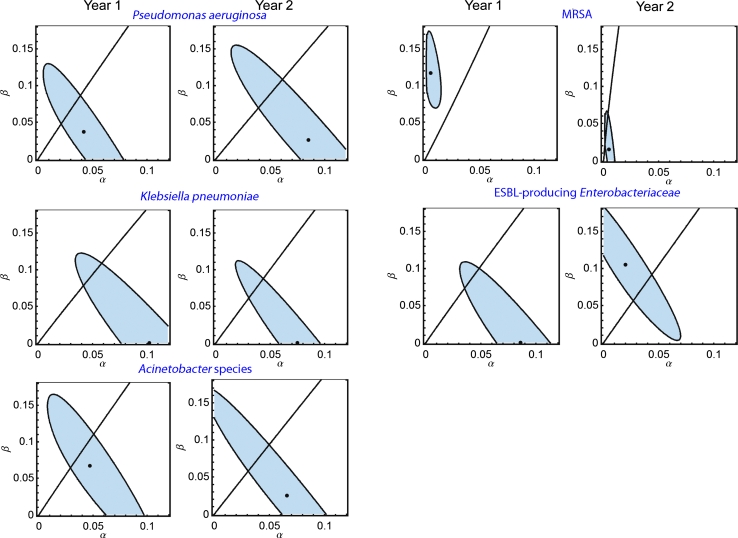
All patients admitted within the study period were included. After a 1-year baseline period, barrier precautions were implemented and the single empirical treatment ceftazidime was changed to mixing (per consecutive patient) of three different regimens (ceftazidime, ciprofloxacin, piperacillin-tazobactam). Markov chain modeling and genotyping were used to determine the effects of interventions on prevalence levels and the relative importance of cross-transmission and antibiotic-associated selection.
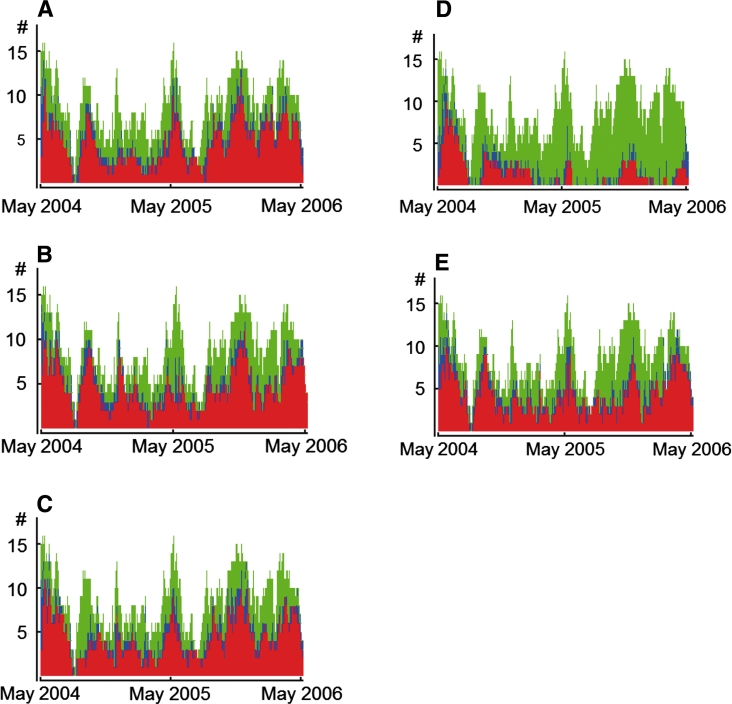
A total of 190 patients were included in year 1 (2,708 patient days, 17,260 cultures) and 167 patients in year 2 (3,384 patient days, 20,580 cultures). In year 1, average daily prevalence rates for methicillin-resistant Staphylococcus aureus (MRSA), extended spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae (excluding Klebsiella pneumoniae), Pseudomonas aeruginosa, gentamicin-resistant K. pneumoniae, and amikacin-resistant Acinetobacter species were 34.0, 61.3, 53.4, 65.7 and 57.1 %. After intervention, ceftazidime usage decreased by 53 %; the use of piperacillin-tazobactam and ciprofloxacin increased 7.2-fold and 4.5-fold, respectively. Adherence to hand hygiene after patient contact was 54 %. These measures were associated with a reduction of MRSA prevalence by 69.8 % (to 10.3 %), mainly because of less cross-transmission (88 % reduction), and of ESBL-producing Enterobacteriaceae prevalence by 10.3 % (non-significantly). In contrast, prevalence levels of the other three pathogens remained unaffected.
The combination of simple infection control measures and antibiotic mixing was highly effective in reducing the prevalence of MRSA, but not of Gram-negative microorganisms.
在越南胡志明市的一家三级转诊医院的破伤风重症监护病房内,量化屏障预防措施和抗生素混合使用对五种耐药微生物的流行和获得的影响。
所有在研究期间入院的患者均被纳入研究。在基线期 1 年后,实施了屏障预防措施,并将单种经验性治疗药物头孢他啶改为三种不同方案(头孢他啶、环丙沙星、哌拉西林他唑巴坦)的混合用药(每连续一位患者)。采用马尔可夫链模型和基因分型来确定干预措施对流行水平的影响,以及交叉传播和抗生素相关选择的相对重要性。
在第 1 年纳入了 190 名患者(2708 个患者日,17260 个培养物),第 2 年纳入了 167 名患者(3384 个患者日,20580 个培养物)。在第 1 年,耐甲氧西林金黄色葡萄球菌(MRSA)、产超广谱β-内酰胺酶(ESBL)的肠杆菌科(不包括肺炎克雷伯菌)、铜绿假单胞菌、庆大霉素耐药肺炎克雷伯菌和阿米卡星耐药不动杆菌的平均日流行率分别为 34.0%、61.3%、53.4%、65.7%和 57.1%。干预后,头孢他啶的使用量减少了 53%;哌拉西林他唑巴坦和环丙沙星的使用量分别增加了 7.2 倍和 4.5 倍。接触患者后进行手部卫生的依从性为 54%。这些措施与 MRSA 流行率降低 69.8%(至 10.3%)相关,主要是因为交叉传播减少了 88%,产 ESBL 的肠杆菌科流行率降低了 10.3%(无统计学意义)。相比之下,其他三种病原体的流行水平没有受到影响。
简单的感染控制措施和抗生素混合使用的组合非常有效地降低了 MRSA 的流行率,但对革兰氏阴性微生物无效。