Graves Patricia M, Makita Leo, Susapu Melinda, Brady Molly A, Melrose Wayne, Capuano Corinne, Zhang Zaixing, Dapeng Luo, Ozaki Masayo, Reeve David, Ichimori Kazuyo, Kazadi Walter M, Michna Frederick, Bockarie Moses J, Kelly-Hope Louise A
Department of Public Health, Tropical Medicine and Rehabilitation Sciences, James Cook University, Cairns and Townsville, Queensland, Australia.
Parasit Vectors. 2013 Jan 11;6:7. doi: 10.1186/1756-3305-6-7.
Lymphatic filariasis (LF) caused by Wuchereria bancrofti is present at high prevalence in some parts of Papua New Guinea. However, there has been no rigorous data-based representative assessment of nationwide prevalence of LF. The LF programme has been daunted by the scope of the problem, and progress on mass drug administration (MDA) has been slow and lacking in resources.
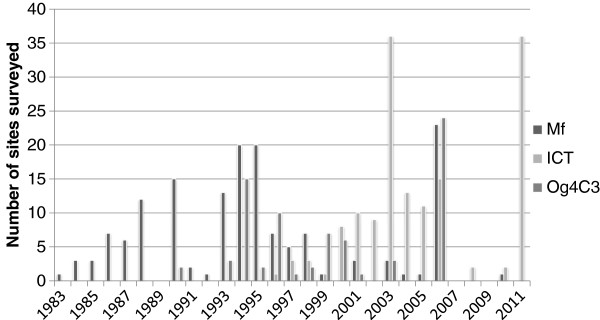
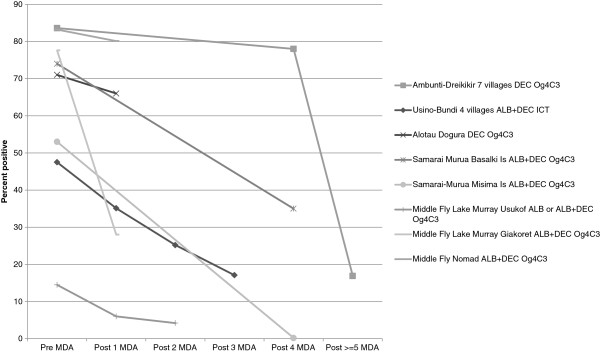
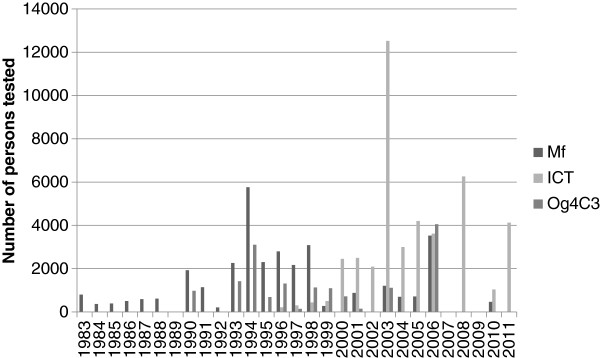
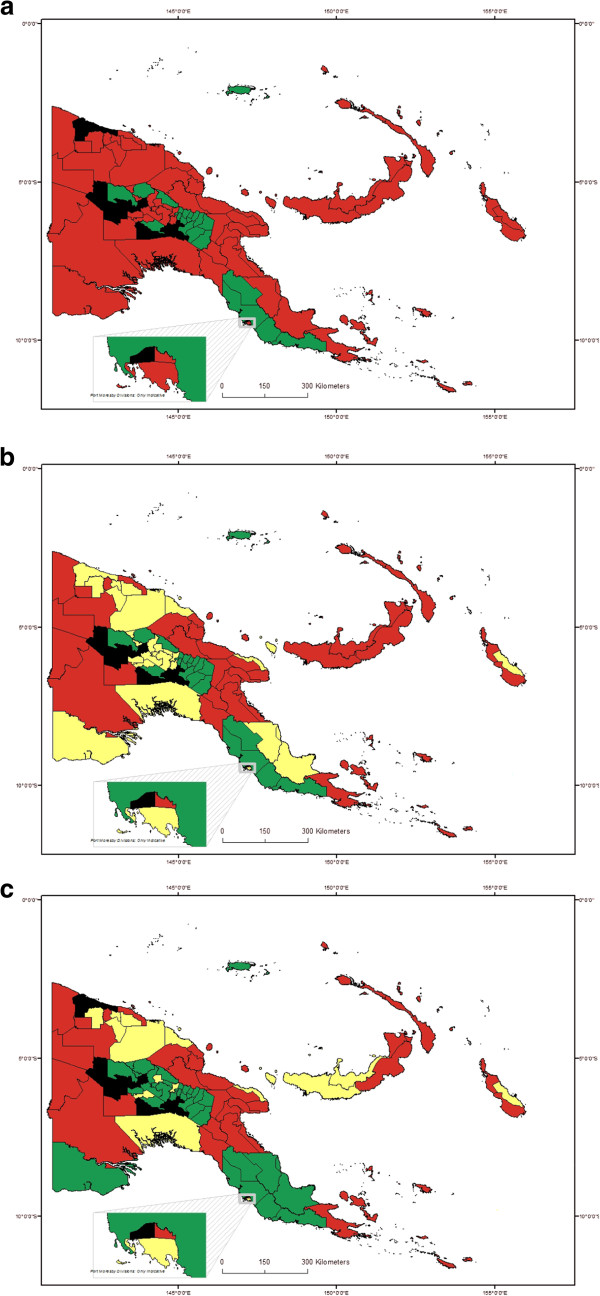
A systematic literature review identified LF surveys in Papua New Guinea between 1980 and 2011. Results were extracted by location, time period and test used (blood slide, immunochromatographic test (ICT) or Og4C3 ELISA) and combined by district. Three criteria schemes based on the Global Programme to Eliminate Lymphatic Filariasis guidelines, with modifications, were developed to classify and prioritize districts by prevalence level. Results of repeated surveys in the same sites were used to investigate the impact of MDA on LF prevalence over the time period.
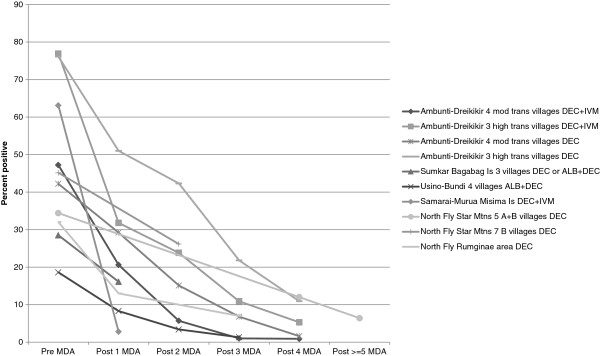
There were 312 distinct survey sites identified in 80 of the 89 districts over the 31-year period. The overall LF prevalence in the sites tested was estimated at 18.5 to 27.5% by blood slide for microfilariae (Mf), 10.1% to 12.9% by ICT and 45.4% to 48.8% by Og4C3. Biases in site selection towards areas with LF, and change in type of assay used, affected the prevalence estimates, but overall decline in prevalence over the time period was observed. Depending on the criteria used, 34 to 36 districts (population 2.7 to 2.9 million) were classed as high endemic (≥5% prevalence), 15 to 25 districts (1.7 to 1.9 million) as low endemic (<5%) and 20 to 31 (1.3 to 2.2 million) as non-endemic. Nine districts (0.7 million) had no information. The strong impact of MDA, especially on microfilaria (Mf) prevalence, was noted in sites with repeat surveys.
This analytical review of past surveys of LF in Papua New Guinea enables better estimation of the national burden, identifies gaps in knowledge, quantifies and locates the population at risk, and can be used to predict the likely impact of MDA and/or vector control. Better targeting of districts by level of prevalence will strengthen the control programme, facilitate monitoring of the disease trend and increase the likelihood of reaching the target of LF elimination by 2020.
由班氏吴策线虫引起的淋巴丝虫病(LF)在巴布亚新几内亚的一些地区高发。然而,目前尚无基于严格数据的全国性LF患病率代表性评估。LF防治项目因问题规模庞大而受阻,大规模药物给药(MDA)进展缓慢且资源匮乏。
通过系统文献回顾,确定了1980年至2011年间巴布亚新几内亚的LF调查。按地点、时间段和所用检测方法(血涂片、免疫层析试验(ICT)或Og4C3酶联免疫吸附测定(ELISA))提取结果,并按地区进行汇总。根据全球消除淋巴丝虫病规划指南制定了三个标准方案,并进行了修改,以按流行程度对地区进行分类和排序。利用同一地点重复调查的结果,研究MDA在该时间段内对LF患病率的影响。
在31年期间,89个地区中的80个地区共确定了312个不同的调查地点。通过血涂片检测微丝蚴(Mf),检测地点的总体LF患病率估计为18.5%至27.5%;通过ICT检测为10.1%至12.9%;通过Og4C3检测为45.4%至48.8%。调查地点选择偏向LF流行地区以及所用检测方法的变化影响了患病率估计,但在该时间段内仍观察到患病率总体下降。根据所用标准,34至36个地区(人口270万至290万)被列为高流行区(患病率≥5%),15至25个地区(170万至190万)为低流行区(患病率<5%),20至31个地区(130万至220万)为非流行区。9个地区(70万人口)无相关信息。在进行重复调查的地点,注意到MDA有显著影响,尤其是对微丝蚴(Mf)患病率的影响。
对巴布亚新几内亚过去LF调查的这一分析性回顾有助于更好地估计国家负担,找出知识空白,量化并确定高危人群,还可用于预测MDA和/或病媒控制的可能影响。根据流行程度对地区进行更精准的定位将加强防控项目,便于监测疾病趋势,并增加到2020年实现消除LF目标的可能性。