Department of Medicine, Lihir Medical Centre, International SOS, Lihir Island, New Ireland Province, Papua New Guinea.
PLoS Negl Trop Dis. 2011 Aug;5(8):e1286. doi: 10.1371/journal.pntd.0001286. Epub 2011 Aug 23.
Annual mass drug administration (MDA) over five years is the WHO's recommended strategy to eliminate lymphatic filariasis (LF). Some experts, however, consider that longer periods of treatment might be necessary in certain high prevalence and transmission environments based upon past unsuccessful field experience and modelling.
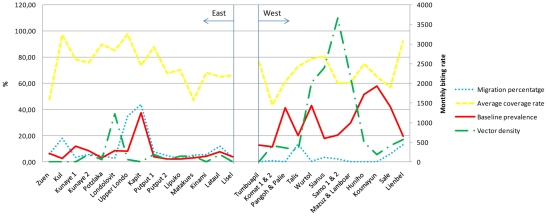
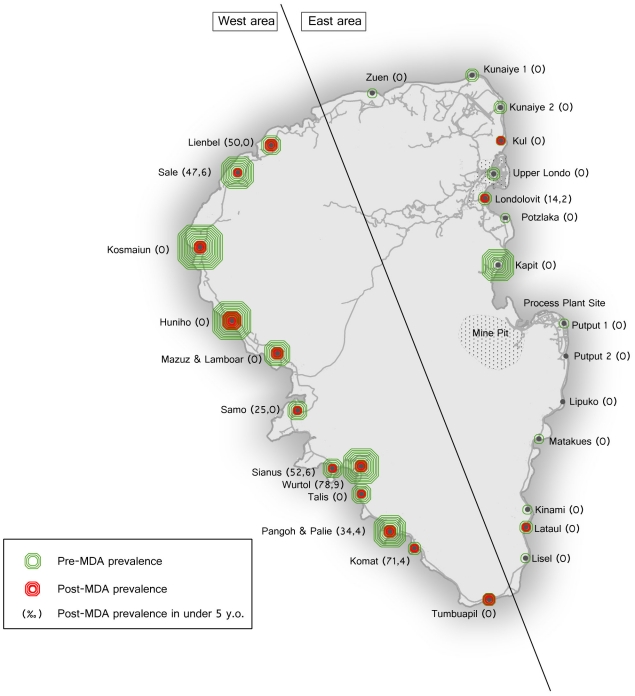
METHODOLOGY/PRINCIPAL FINDINGS: To evaluate predictors of success in a LF control program we conducted an ecological study during a pre-existing MDA program. We studied 27 villages in Lihir Island, Papua New Guinea, from two areas with different infection rates before MDA. We undertook surveys to collect information on variables potentially having an influence on the outcome of the program, including epidemiological (baseline prevalence of infection, immigration rate), entomological (vector density) and operational (treatment coverage, vector control strategies) variables. The success in a village was defined using variables related to the infection (circulating filarial antigenemia prevalence < 1%) and transmission (antigenemia prevalence < 1 in 1000 children born since start of MDA). 8709 people were involved in the MDA program and average coverage rates were around 70%. The overall prevalence of filariasis fell from an initial 17.91% to 3.76% at round 5 (p < 0.001). Viewed on a village by village basis, 12/27 (44%) villages achieved success. In multivariate analysis, low baseline prevalence was the only factor predicting both success in reducing infection rates (OR 19,26; CI 95% 1,12 to 331,82) and success in preventing new infections (OR 27,44; CI 95% 1,05 to 719,6). Low vector density and the use of an optimal vector control strategy were also associated with success in reducing infection rates, but this did not reach statistical significance.
CONCLUSIONS/SIGNIFICANCE: Our results provide the data that supports the recommendation that high endemic areas may require longer duration MDA programs, or alternative control strategies.
世界卫生组织建议每年进行五年大规模药物治疗(MDA),以消除淋巴丝虫病(LF)。然而,一些专家认为,基于过去不成功的实地经验和建模,在某些高流行率和传播环境中,可能需要更长时间的治疗。
方法/主要发现:为了评估 LF 控制规划成功的预测因素,我们在现有的 MDA 规划期间进行了一项生态研究。我们研究了巴布亚新几内亚利希尔岛的 27 个村庄,这些村庄来自 MDA 前两个具有不同感染率的地区。我们进行了调查,收集了可能对规划结果产生影响的变量信息,包括流行病学(基线感染率、移民率)、昆虫学(媒介密度)和操作变量(治疗覆盖率、媒介控制策略)。村庄的成功定义为与感染(循环丝状抗原血症患病率<1%)和传播(自 MDA 开始以来出生的 1000 名儿童中抗原血症患病率<1/1000)相关的变量。有 8709 人参与了 MDA 规划,平均覆盖率约为 70%。总体丝虫病患病率从最初的 17.91%下降到第 5 轮的 3.76%(p<0.001)。从村庄到村庄来看,27 个村庄中有 12 个(44%)取得了成功。在多变量分析中,低基线患病率是预测降低感染率成功(OR 19.26;95%CI 1.12 至 331.82)和预防新感染成功(OR 27.44;95%CI 1.05 至 719.6)的唯一因素。低媒介密度和使用最佳媒介控制策略也与降低感染率的成功相关,但这并未达到统计学意义。
结论/意义:我们的结果提供了支持高流行地区可能需要更长时间 MDA 规划或替代控制策略的建议的数据。