Department of Nutrition and Dietetics, King's College Hospital, London, UK.
BMJ Open. 2013 Jan 11;3(1):e002173. doi: 10.1136/bmjopen-2012-002173.
Refeeding syndrome is a potentially life-threatening condition characterised by severe intracellular electrolyte shifts, acute circulatory fluid overload and organ failure. The initial symptoms are non-specific but early clinical features are severely low-serum electrolyte concentrations of potassium, phosphate or magnesium. Risk factors for the syndrome include starvation, chronic alcoholism, anorexia nervosa and surgical interventions that require lengthy periods of fasting. The causes of the refeeding syndrome are excess or unbalanced enteral, parenteral or oral nutritional intake. Prevention of the syndrome includes identification of individuals at risk, controlled hypocaloric nutritional intake and supplementary electrolyte replacement.
To determine the occurrence of refeeding syndrome in adults commenced on artificial nutrition support.
Prospective cohort study.
Large, single site university teaching hospital. Recruitment period 2007-2009.
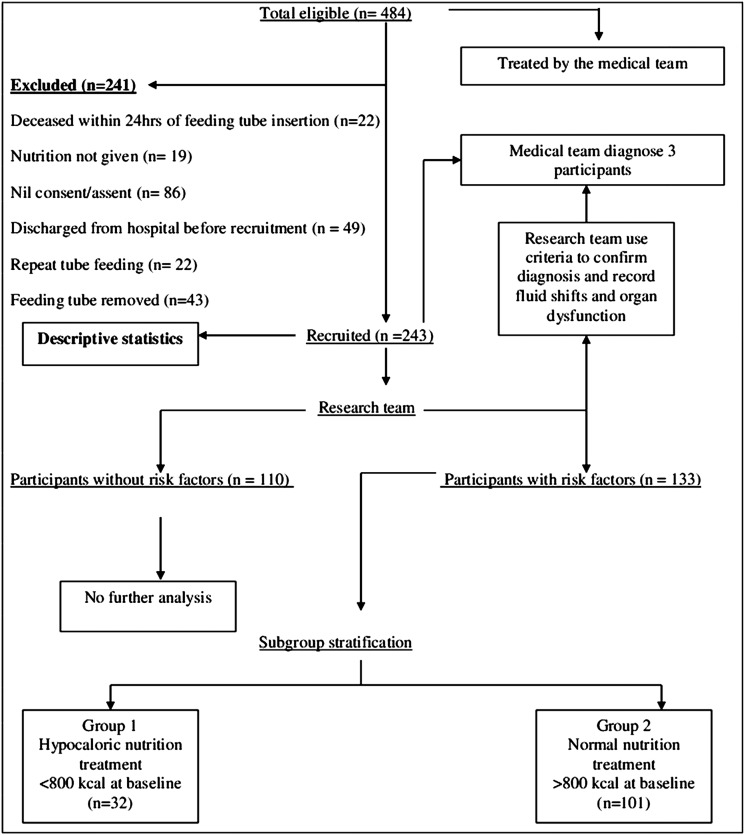
243 adults started on artificial nutrition support for the first time during that admission recruited from wards and intensive care.
occurrence of the refeeding syndrome. Secondary outcome: analysis of the risk factors which predict the refeeding syndrome. Tertiary outcome: mortality due to refeeding syndrome and all-cause mortality.
133 participants had one or more of the following risk factors: body mass index <16-18.5≥(kg/m(2)), unintentional weight loss >15% in the preceding 3-6 months, very little or no nutritional intake >10 days, history of alcohol or drug abuse and low baseline levels of serum potassium, phosphate or magnesium prior to recruitment. Poor nutritional intake for more than 10 days, weight loss >15% prior to recruitment and low-serum magnesium level at baseline predicted the refeeding syndrome with a sensitivity of 66.7%: specificity was >80% apart from weight loss of >15% which was 59.1%. Baseline low-serum magnesium was an independent predictor of the refeeding syndrome (p=0.021). Three participants (2% 3/243) developed severe electrolyte shifts, acute circulatory fluid overload and disturbance to organ function following artificial nutrition support and were diagnosed with refeeding syndrome. There were no deaths attributable to the refeeding syndrome, but (5.3% 13/243) participants died during the feeding period and (28% 68/243) died during hospital admission. Death of these participants was due to cerebrovascular accident, traumatic injury, respiratory failure, organ failure or end-of-life causes.
Refeeding syndrome was a rare, survivable phenomenon that occurred during hypocaloric nutrition support in participants identified at risk. Independent predictors for refeeding syndrome were starvation and baseline low-serum magnesium concentration. Intravenous carbohydrate infusion prior to artificial nutrition support may have precipitated the onset of the syndrome.
再喂养综合征是一种潜在的危及生命的疾病,其特征为严重的细胞内电解质转移、急性循环液超负荷和器官衰竭。最初的症状是非特异性的,但早期的临床特征是严重的血清电解质浓度低钾、磷或镁。该综合征的危险因素包括饥饿、慢性酒精中毒、神经性厌食症和需要长时间禁食的手术干预。再喂养综合征的原因是肠内、肠外或口服营养摄入过多或不平衡。该综合征的预防包括识别处于危险中的个体、控制低热量营养摄入和补充电解质替代物。
确定首次接受人工营养支持的成年人中再喂养综合征的发生情况。
前瞻性队列研究。
大型单一站点大学教学医院。招募期为 2007 年至 2009 年。
243 名首次在该病房和重症监护室接受人工营养支持的成年人被招募。
再喂养综合征的发生情况。次要结局:分析预测再喂养综合征的危险因素。三级结局:再喂养综合征相关死亡率和全因死亡率。
133 名参与者存在以下一种或多种危险因素:体重指数<16-18.5≥(kg/m(2))、前 3-6 个月体重非故意丢失>15%、营养摄入非常少或>10 天无摄入、有酒精或药物滥用史和招募前血清钾、磷或镁基线水平低。营养摄入不良>10 天、招募前体重丢失>15%和血清镁水平低是再喂养综合征的预测指标,其敏感性为 66.7%:特异性>80%,除了>15%的体重丢失为 59.1%。基线低血清镁是再喂养综合征的独立预测因素(p=0.021)。3 名参与者(2% 3/243)在接受人工营养支持后出现严重的电解质转移、急性循环液超负荷和器官功能障碍,并被诊断为再喂养综合征。没有因再喂养综合征导致的死亡,但(5.3% 13/243)名参与者在喂养期间死亡,(28% 68/243)名参与者在住院期间死亡。这些参与者的死亡是由于脑血管意外、创伤性损伤、呼吸衰竭、器官衰竭或生命末期原因。
再喂养综合征是一种罕见的、可存活的现象,在有风险的参与者中,在低热量营养支持期间发生。再喂养综合征的独立预测因子是饥饿和基线低血清镁浓度。在开始人工营养支持之前进行静脉内碳水化合物输注可能会引发该综合征的发生。