Department of Radiation Oncology, Memorial Sloan-Kettering Cancer Center New York, NY, USA.
Front Oncol. 2013 Jan 3;2:208. doi: 10.3389/fonc.2012.00208. eCollection 2012.
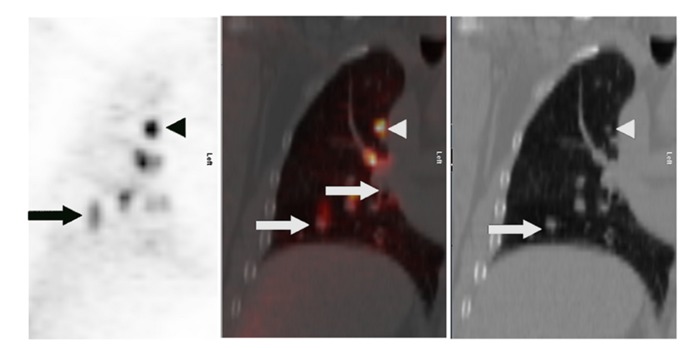
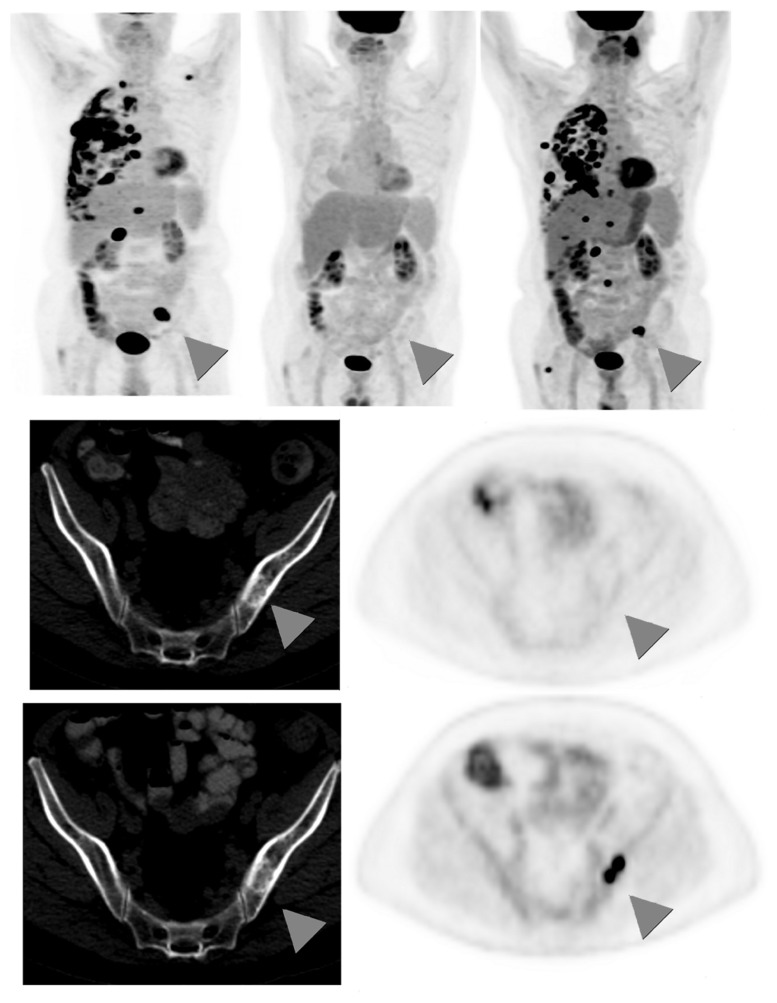
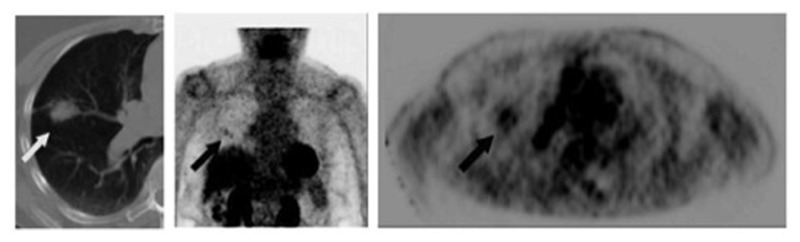
The integral role of positron-emission tomography (PET) using the glucose analog tracer fluorine-18 fluorodeoxyglucose (FDG) in the staging of non-small cell lung cancer (NSCLC) is well established. Evidence is emerging for the role of PET in response assessment to neoadjuvant therapy, combined-modality therapy, and early detection of recurrence. Here, we review the current literature on these aspects of PET in the management of NSCLC. FDG-PET, particularly integrated (18)F-FDG-PET/CT, scans have become a standard test in the staging of local tumor extent, mediastinal lymph node involvement, and distant metastatic disease in NSCLC. (18)F-FDG-PET sensitivity is generally superior to computed tomography (CT) scans alone. Local tumor extent and T stage can be more accurately determined with FDG-PET in certain cases, especially in areas of post-obstructive atelectasis or low CT density variation. FDG-PET sensitivity is decreased in tumors <1 cm, at least in part due to respiratory motion. False-negative results can occur in areas of low tumor burden, e.g., small lymph nodes or ground-glass opacities. (18)F-FDG-PET-CT nodal staging is more accurate than CT alone, as hilar and mediastinal involvement is often detected first on (18)F-FDG-PET scan when CT criteria for malignant involvement are not met. (18)F-FDG-PET scans have widely replaced bone scintography for assessing distant metastases, except for the brain, which still warrants dedicated brain imaging. (18)F-FDG uptake has also been shown to vary between histologies, with adenocarcinomas generally being less FDG avid than squamous cell carcinomas. (18)F-FDG-PET scans are useful to detect recurrences, but are currently not recommended for routine follow-up. Typically, patients are followed with chest CT scans every 3-6 months, using (18)F-FDG-PET to evaluate equivocal CT findings. As high (18)F-FDG uptake can occur in infectious, inflammatory, and other non-neoplastic conditions, (18)F-FDG-PET-positive findings require pathological confirmation in most cases. There is increased interest in the prognostic and predictive role of FDG-PET scans. Studies show that absence of metabolic response to neoadjuvant therapy correlates with poor pathologic response, and a favorable (18)F-FDG-PET response appears to be associated with improved survival. Further work is underway to identify subsets of patients that might benefit individualized management based on FDG-PET.
正电子发射断层扫描(PET)使用葡萄糖类似物示踪剂氟-18 氟脱氧葡萄糖(FDG)在非小细胞肺癌(NSCLC)分期中的整体作用已得到充分证实。越来越多的证据表明,PET 在新辅助治疗、联合治疗和早期复发检测的反应评估中具有作用。在这里,我们回顾了 PET 在 NSCLC 管理中的这些方面的当前文献。FDG-PET,特别是整合的(18)F-FDG-PET/CT 扫描,已成为 NSCLC 局部肿瘤范围、纵隔淋巴结受累和远处转移疾病分期的标准测试。(18)F-FDG-PET 的敏感性通常优于单独的计算机断层扫描(CT)扫描。在某些情况下,FDG-PET 可更准确地确定局部肿瘤范围和 T 分期,特别是在阻塞性肺不张或 CT 密度变化较小的区域。由于呼吸运动,直径<1cm 的肿瘤的 FDG 摄取减少,至少部分原因是呼吸运动。在肿瘤负荷较低的区域(例如小淋巴结或磨玻璃样混浊),可能会出现假阴性结果。(18)F-FDG-PET-CT 淋巴结分期比单独 CT 更准确,因为当 CT 不符合恶性受累标准时,通常首先在(18)F-FDG-PET 扫描上检测到肺门和纵隔受累。(18)F-FDG-PET 扫描已广泛取代骨闪烁显像术来评估远处转移,除了大脑,大脑仍需要专门的脑部成像。(18)F-FDG 摄取也表现出组织学之间的差异,腺癌的 FDG 摄取通常低于鳞状细胞癌。(18)F-FDG-PET 扫描可用于检测复发,但目前不建议常规随访。通常,患者每 3-6 个月进行一次胸部 CT 扫描,使用(18)F-FDG-PET 评估不确定的 CT 发现。由于高(18)F-FDG 摄取可发生在感染、炎症和其他非肿瘤性疾病中,因此大多数情况下,(18)F-FDG-PET 阳性发现需要病理证实。人们对 FDG-PET 扫描的预后和预测作用越来越感兴趣。研究表明,对新辅助治疗无代谢反应与不良病理反应相关,而有利的(18)F-FDG-PET 反应似乎与改善生存相关。正在进行进一步的工作,以确定可能基于 FDG-PET 受益于个体化管理的患者亚组。