General Medicine Division, Department of Medicine, Massachusetts General Hospital, Boston, MA 02114, USA.
JAMA Intern Med. 2013 Feb 11;173(3):189-95. doi: 10.1001/jamainternmed.2013.1604.
Homeless persons experience excess mortality, but US-based studies on this topic are outdated or lack information about causes of death. To our knowledge, no studies have examined shifts in causes of death for this population over time.
We assessed all-cause and cause-specific mortality rates in a cohort of 28 033 adults 18 years or older who were seen at Boston Health Care for the Homeless Program from January 1, 2003, through December 31, 2008. Deaths were identified through probabilistic linkage to the Massachusetts death occurrence files. We compared mortality rates in this cohort with rates in the 2003-2008 Massachusetts population and a 1988-1993 cohort of homeless adults in Boston using standardized rate ratios with 95% confidence intervals.
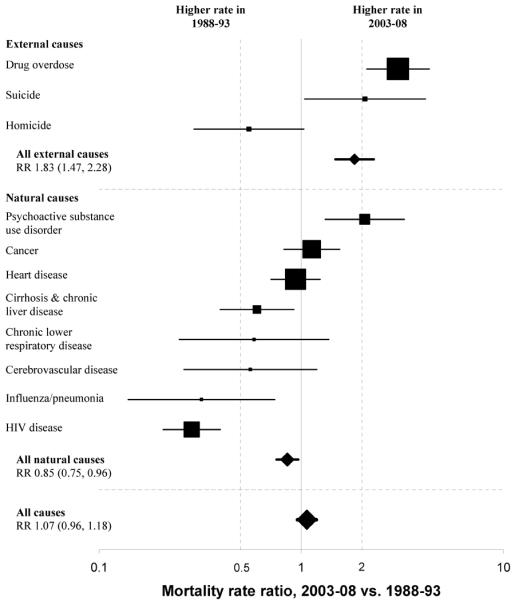
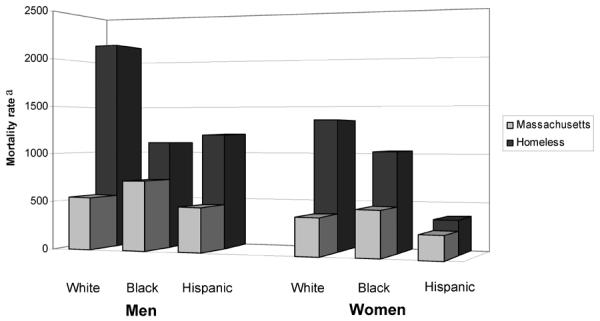
A total of 1302 deaths occurred during 90 450 person-years of observation. Drug overdose (n = 219), cancer (n = 206), and heart disease (n = 203) were the major causes of death. Drug overdose accounted for one-third of deaths among adults younger than 45 years. Opioids were implicated in 81% of overdose deaths. Mortality rates were higher among whites than nonwhites. Compared with Massachusetts adults, mortality disparities were most pronounced among younger individuals, with rates about 9-fold higher in 25- to 44-year-olds and 4.5-fold higher in 45- to 64-year-olds. In comparison with 1988-1993 rates, reductions in deaths from human immunodeficiency virus (HIV) were offset by 3- and 2-fold increases in deaths owing to drug overdose and psychoactive substance use disorders, resulting in no significant difference in overall mortality.
The all-cause mortality rate among homeless adults in Boston remains high and unchanged since 1988 to 1993 despite a major interim expansion in clinical services. Drug overdose has replaced HIV as the emerging epidemic. Interventions to reduce mortality in this population should include behavioral health integration into primary medical care, public health initiatives to prevent and reverse drug overdose, and social policy measures to end homelessness.
无家可归者的死亡率过高,但美国关于这一主题的研究已经过时或缺乏有关死亡原因的信息。据我们所知,尚无研究探讨随着时间的推移,该人群的死亡原因发生了怎样的变化。
我们评估了 2003 年 1 月 1 日至 2008 年 12 月 31 日期间在波士顿卫生保健为无家可归者项目就诊的 28033 名 18 岁或以上成年人的全因和特定原因死亡率。通过概率链接到马萨诸塞州死亡事件档案来确定死亡。我们使用标准化比率比和 95%置信区间,将该队列的死亡率与马萨诸塞州 2003-2008 年人群的死亡率和 1988-1993 年波士顿无家可归成年人队列的死亡率进行了比较。
在 90450 人年的观察期间,共发生 1302 例死亡。药物过量(n=219)、癌症(n=206)和心脏病(n=203)是主要死亡原因。药物过量占 45 岁以下成年人死亡人数的三分之一。阿片类药物在 81%的过量死亡中被牵连。白种人死亡率高于非白种人。与马萨诸塞州成年人相比,死亡率差异在年轻人群中最为明显,25-44 岁人群的死亡率高 9 倍,45-64 岁人群的死亡率高 4.5 倍。与 1988-1993 年的死亡率相比,由于药物过量和精神活性物质使用障碍导致的死亡人数增加了 3 倍和 2 倍,艾滋病毒导致的死亡人数减少,因此总体死亡率没有显著差异。
尽管在这期间临床服务大幅扩展,但自 1988 年至 1993 年以来,波士顿无家可归成年人的全因死亡率仍然很高且保持不变。药物过量已取代艾滋病毒成为新出现的流行疾病。为降低该人群的死亡率,应将行为健康纳入初级医疗保健,制定公共卫生计划以预防和扭转药物过量,以及采取社会政策措施以消除无家可归现象。