Romero R, Avila C, Santhanam U, Sehgal P B
Department of Obstetrics and Gynecology, Yale University School of Medicine, New Haven, Connecticut 06510.
J Clin Invest. 1990 May;85(5):1392-400. doi: 10.1172/JCI114583.
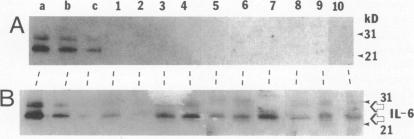
To evaluate whether IL-6 participates in the host response to intrauterine infection, we studied IL-6 bioactivity and isoforms in amniotic fluid (AF). Two different assays for IL-6 were used: the hepatocyte stimulating factor assay (in Hep3B2 cells) and the SDS-PAGE/immunoblot assay. IL-6 determinations were performed in 205 AF samples. Samples were obtained from patients in the midtrimester of pregnancy (n = 25), at term with no labor (n = 31), at term in active labor (n = 40), and from patients in preterm labor (n = 109). Higher AF IL-6 levels were observed in women in preterm labor with intraamniotic infection than in women in preterm labor without intraamniotic infection (median = 375 ng/ml, range = 30-5000 ng/ml vs. median = 1.5 ng/ml, range = 0-500, respectively, P less than 0.0001). The 23-25- and 28-30-kD IL-6 species could be readily detected in SDS-PAGE immunoblots performed directly on 10-microliters aliquots of AF from patients with intraamniotic infection. Among women in preterm labor with culture-negative AF, those who failed to respond to subsequent tocolytic treatment had higher AF IL-6 concentrations than those who responded to therapy (median = 50 ng/ml vs. median = 1.2 ng/ml, respectively, P less than 0.05). Only low levels of IL-6 were detected in AF obtained from normal women in the midtrimester and third trimester of pregnancy. Decidual tissue explants obtained from the placentas of women undergoing elective cesarean section at term without labor (n = 11) produced IL-6 in response to bacterial endotoxin. In a pilot study, AF IL-6 was determined in 56 consecutive women admitted with preterm labor. All patients (n = 10) with elevated AF IL-6 (cutoff = 46 ng/ml) delivered a premature neonate. 4 of these 10 patients had positive AF cultures for microorganisms. These studies implicate IL-6 in the host response to intrauterine infection and suggest that evaluation of AF IL-6 levels may have diagnostic and prognostic value in the management of women in preterm labor.
为评估白细胞介素-6(IL-6)是否参与宿主对宫内感染的反应,我们研究了羊水(AF)中的IL-6生物活性和异构体。采用了两种不同的IL-6检测方法:肝细胞刺激因子检测法(在Hep3B2细胞中)和十二烷基硫酸钠-聚丙烯酰胺凝胶电泳/免疫印迹检测法。对205份AF样本进行了IL-6测定。样本取自妊娠中期的患者(n = 25)、足月未临产的患者(n = 31)、足月临产的患者(n = 40)以及早产患者(n = 109)。与未发生羊膜腔内感染的早产女性相比,发生羊膜腔内感染的早产女性羊水IL-6水平更高(中位数分别为375 ng/ml,范围为30 - 5000 ng/ml与中位数为1.5 ng/ml,范围为0 - 500,P < 0.0001)。在对羊膜腔内感染患者10微升AF等分试样直接进行的十二烷基硫酸钠-聚丙烯酰胺凝胶电泳免疫印迹中,可轻易检测到23 - 25 kD和28 - 30 kD的IL-6亚型。在AF培养阴性的早产女性中,对后续宫缩抑制剂治疗无反应者的羊水IL-6浓度高于有反应者(中位数分别为50 ng/ml与中位数为1.2 ng/ml,P < 0.05)。在妊娠中期和晚期的正常女性的羊水中仅检测到低水平的IL-6。从足月未临产接受择期剖宫产的女性(n = 11)的胎盘获取的蜕膜组织外植体对细菌内毒素有反应并产生IL-6。在一项初步研究中,对56例连续因早产入院的女性测定了羊水IL-6。所有羊水IL-6升高(临界值 = 46 ng/ml)的患者(n = 10)均分娩了早产儿。这10例患者中有4例羊水微生物培养呈阳性。这些研究表明IL-6参与宿主对宫内感染的反应,并提示评估羊水IL-6水平可能对早产女性的管理具有诊断和预后价值。