Department of Epidemiology and the Welch Center for Prevention, Epidemiology and Clinical Research, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21287, USA.
Am J Kidney Dis. 2013 May;61(5):716-22. doi: 10.1053/j.ajkd.2012.11.048. Epub 2013 Jan 20.
Our objective was to quantify short-term total within-person variability in standard and nontraditional kidney measures using national data.
Repeated examination study of serum and urine kidney measures.
SETTING & PARTICIPANTS: Participants 18 years or older in the Third National Health and Nutrition Examination Survey (NHANES III) who had repeated blood and urine samples collected during visits occurring approximately 18 days apart.
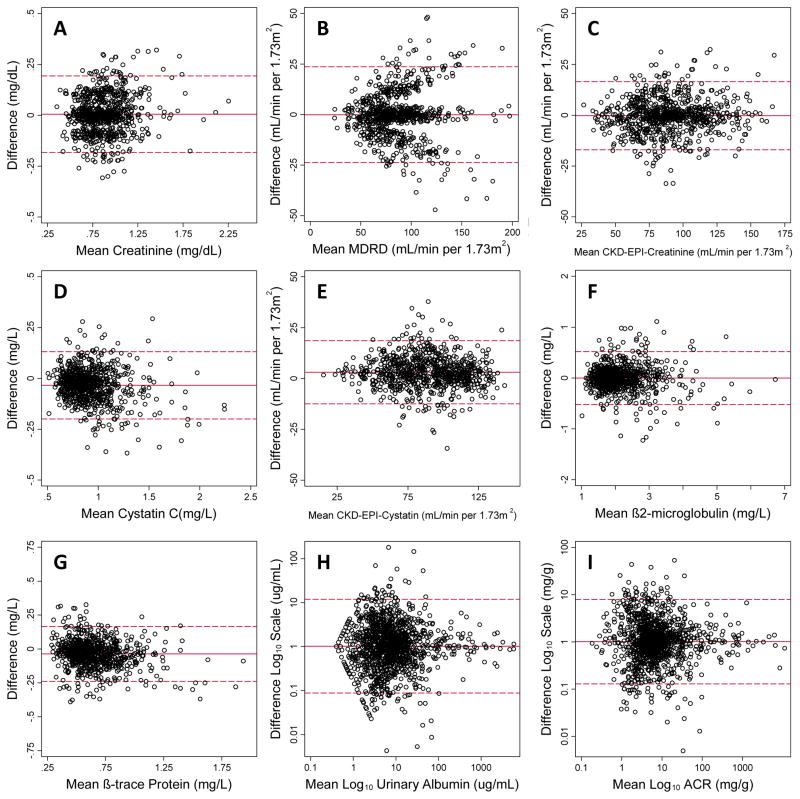
Standardized serum creatinine, standardized cystatin C, β-trace protein (BTP), β(2)-microglobulin (B2M), and urine albumin and creatinine. We calculated the within-person coefficient of variation (CV(w)), which includes both biological and analytical variability. We also evaluated the impact of variability on estimates of the prevalence of reduced estimated glomerular filtration rate and albuminuria.
Serum cystatin C level demonstrated the lowest short-term within-person variability (CV(w) = 6.8%). Serum creatinine and B2M levels (CV(w) = 7.6% and 8.4%, respectively) also had low variability. BTP level had the most variability of the serum markers (CV(w) = 11.6%). As expected, urine albumin and urine creatinine measurements showed high variability (CV(w) >30% for both); however, albumin-creatinine ratio performed much better than either measure alone, with CV(w) of 11.3%. The effect of short-term variability on the prevalence of reduced estimated glomerular filtration rate was moderate, with an ~20% lower prevalence when defined based on single measurements compared to repeated application of the same test approximately 18 days apart. Repeated testing for albuminuria had a larger effect, showing a 33% lower prevalence of albuminuria when repeated testing was applied.
Only 2 measurements available. General population with low prevalence of kidney disease.
Our results suggest that creatinine, cystatin C, and B2M levels have similarly low short-term variability. BTP level was more variable compared with the other serum filtration markers. Urine albumin and creatinine levels were highly variable and may benefit from repeated assessments to reduce the misclassification of albuminuria.
本研究旨在利用国家数据量化标准和非传统肾脏指标的短期个体内总变异性。
血清和尿液肾脏指标的重复检测研究。
在第三次全国健康和营养调查(NHANES III)中,年龄在 18 岁或以上的参与者,他们在大约相隔 18 天的访问中重复采集血液和尿液样本。
标准化血清肌酐、标准化胱抑素 C、β-痕迹蛋白(BTP)、β(2)-微球蛋白(B2M)以及尿液白蛋白和肌酐。我们计算了个体内变异系数(CV(w)),它包括生物学和分析变异性。我们还评估了变异性对估算肾小球滤过率降低和蛋白尿患病率估计的影响。
血清胱抑素 C 水平的个体内短期变异性最低(CV(w) = 6.8%)。血清肌酐和 B2M 水平(CV(w)分别为 7.6%和 8.4%)的变异性也较低。BTP 水平的血清标志物变异性最大(CV(w) = 11.6%)。正如预期的那样,尿液白蛋白和尿液肌酐测量值显示出很高的变异性(两者的 CV(w)均大于 30%);然而,白蛋白-肌酐比值的表现明显优于单独使用任何一种测量值,其 CV(w)为 11.3%。短期变异性对估算肾小球滤过率降低的患病率的影响适中,与基于单次测量定义的患病率相比,大约 18 天重复应用相同的测试时,患病率降低约 20%。反复检测蛋白尿的效果更大,当应用重复检测时,蛋白尿的患病率降低 33%。
只有 2 次测量值可用。具有低肾脏疾病患病率的一般人群。
我们的研究结果表明,肌酐、胱抑素 C 和 B2M 水平具有相似的短期变异性低。BTP 水平与其他血清滤过标志物相比更具变异性。尿液白蛋白和肌酐水平高度可变,可能受益于重复评估以减少蛋白尿的错误分类。