Department of Clinical Pharmacy and Pharmacology, University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands.
Second University of Naples, Naples, Italy.
Diabetes Obes Metab. 2022 Jun;24(6):983-990. doi: 10.1111/dom.14660. Epub 2022 Feb 21.
To test whether a screening approach with more flexible urinary albumin creatinine ratio (UACR) and estimated glomerular filtration rate (eGFR) thresholds would decrease screen failure rate without negatively impacting on the event rate and overall study duration.
We performed a post-hoc analysis of the ALTITUDE trial. We selected participants randomized to placebo with a UACR of >300 mg/g and an eGFR between 30 mL/min/1.73 m and 60 mL/min/1.73 m at the first visit (pre-screening) for the trial. We then used less stringent lower UACR and higher eGFR thresholds for the following qualifying visit. For each scenario we calculated the number of eligible participants, the number of renal and cardiovascular endpoints, and the event rates. Based on this, we performed simulations for a future trial and estimated the duration of enrolment and total duration of this trial.
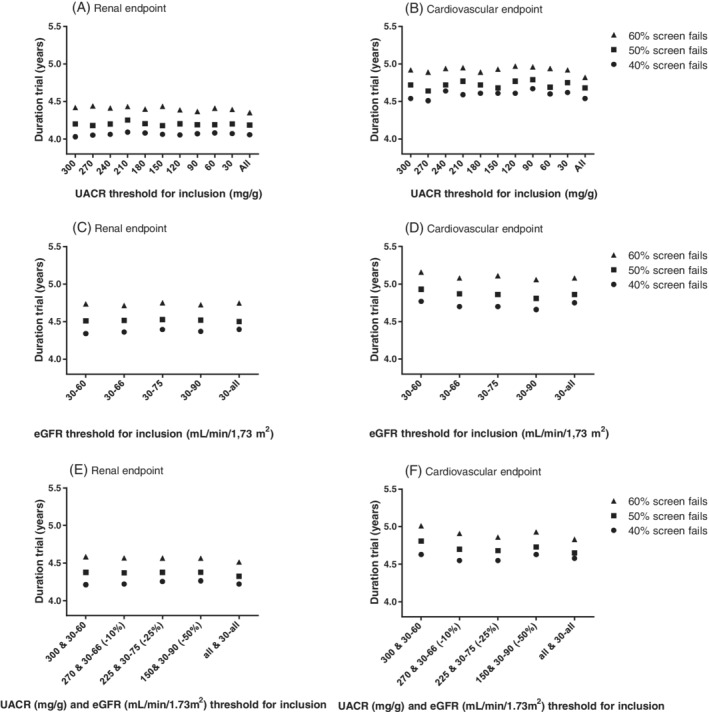
The base scenario consisted of 848 participants (median UACR 1239 mg/g; median eGFR 44 mL/min/1.73 m ). Lowering the UACR and/or raising eGFR qualification thresholds increased the number of eligible participants, decreased screen failures and resulted in only a modest decrease in renal and cardiovascular event rates. For example, relaxing the UACR criterion from 300 mg/g to 210 mg/g at the qualifying visit, increased the number of eligible patients from 848 to 923, and increased the number of renal events from 117 to 122 events. The event rate showed a moderate decrease from 5.6 (4.6-6.7) events per 100 patient-years to 5.3 (4.4-6.4) events per 100 patient-years. In simulations, lowering the UACR and raising eGFR thresholds for inclusion accelerated patient enrolment and did not increase in the overall trial duration.
More flexible albuminuria and eGFR-based inclusion criteria, in participants who met the inclusion criteria of a trial based on pre-screening values prior to the clinical trial, decreases screen failure rates and accelerated patient enrolment leading to more efficient trial conduct without impacting the overall trial duration.
检验更为灵活的尿白蛋白肌酐比值(UACR)和估算肾小球滤过率(eGFR)界值筛查方法是否能在不影响事件发生率和总研究持续时间的情况下降低筛查失败率。
我们对 ALTITUDE 试验进行了事后分析。我们选择了在首次访视(预筛查)时 UACR>300mg/g 且 eGFR 在 30mL/min/1.73m2 至 60mL/min/1.73m2 之间被随机分配至安慰剂的参与者进行分析。然后,我们在下一次符合条件的访视中使用更为宽松的较低 UACR 和较高 eGFR 界值。对于每种情况,我们计算了合格参与者的数量、肾脏和心血管终点的数量以及事件发生率。基于此,我们对未来试验进行了模拟,并估计了入组时间和该试验总持续时间。
基础方案包含 848 名参与者(UACR 中位数为 1239mg/g;eGFR 中位数为 44mL/min/1.73m2)。降低 UACR 和/或提高 eGFR 资格界值增加了合格参与者的数量,降低了筛查失败率,仅导致肾脏和心血管事件发生率适度降低。例如,将符合条件的访视中的 UACR 标准从 300mg/g 放宽至 210mg/g,使合格患者的数量从 848 例增加至 923 例,肾脏事件数量从 117 例增加至 122 例。事件发生率从每 100 患者-年 5.6(4.6-6.7)个事件适度下降至每 100 患者-年 5.3(4.4-6.4)个事件。在模拟中,降低 UACR 和提高纳入的 eGFR 界值加速了患者入组,且不会增加总试验持续时间。
在参加临床试验之前,基于预筛查值,对符合试验纳入标准的参与者使用更为灵活的基于蛋白尿和 eGFR 的纳入标准,可以降低筛查失败率并加速患者入组,从而提高试验效率,且不会影响总试验持续时间。