School of Public Health, Shandong University, Jinan, Shandong Province, China.
PLoS One. 2013;8(1):e51990. doi: 10.1371/journal.pone.0051990. Epub 2013 Jan 16.
In 2009, the Chinese Ministry of Health recommended scale-up of routine neonatal hearing screening - previously performed primarily only in select urban hospitals - throughout the entire country.
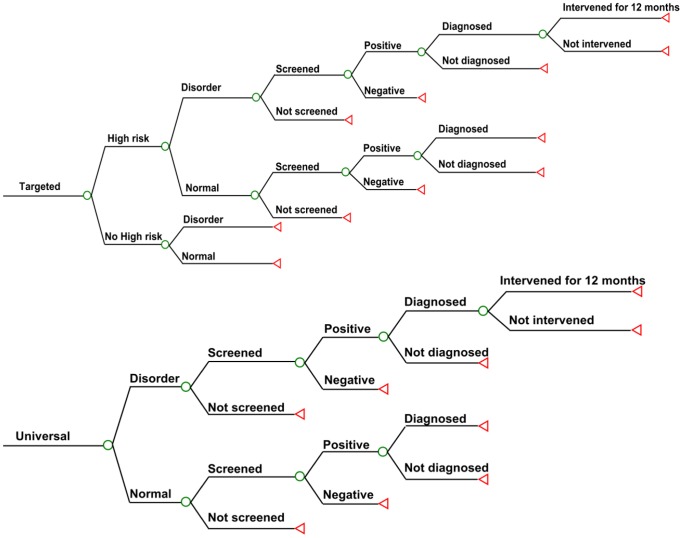
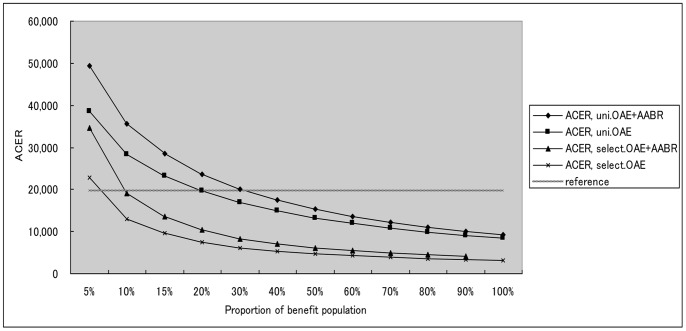
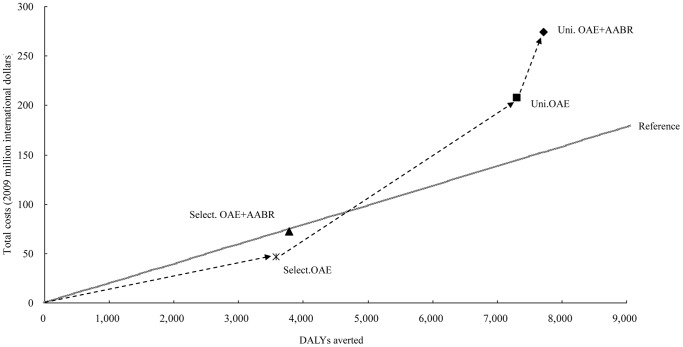
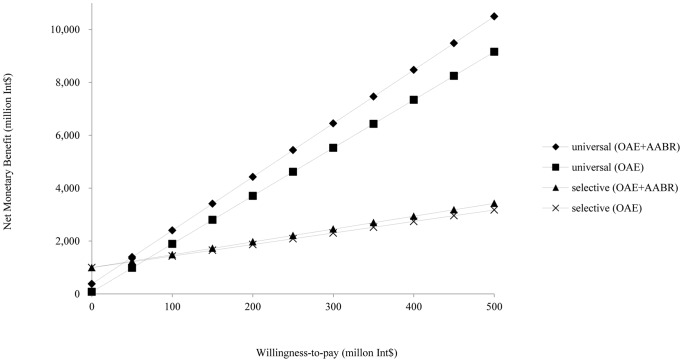
A decision analytical model for a simulated population of all live births in china was developed to compare the costs and health effects of five mutually exclusive interventions: 1) universal screening using Otoacoustic Emission (OAE) and Automated Auditory Brainstem Response (AABR); 2) universal OAE; 3) targeted OAE and AABR; 4) targeted OAE; and 5) no screening. Disability-Adjusted Life Years (DALYs) were calculated for health effects.
Based on the cost-effectiveness and potential health outcomes, the optimal path for scale-up would be to start with targeted OAE and then expand to universal OAE and universal OAE plus AABR. Accessibility of screening, diagnosis, and intervention services significantly affect decision of the options.
In conclusion, to achieve cost-effectiveness and best health outcomes of the NHS program, the accessibility of screening, diagnosis, and intervention services should be expanded to reach a larger population. The results are thus expected to be of particular benefit in terms of the 'rolling out' of the national plan.
2009 年,中国卫生部建议在全国范围内扩大常规新生儿听力筛查的范围——此前主要只在一些选定的城市医院进行。
为模拟中国所有活产儿人群,我们开发了一个决策分析模型,用于比较以下五种互斥干预措施的成本和健康效果:1)使用耳声发射(OAE)和自动听性脑干反应(AABR)的普遍筛查;2)普遍 OAE 筛查;3)有针对性的 OAE 和 AABR 筛查;4)有针对性的 OAE 筛查;5)不进行筛查。使用残疾调整生命年(DALY)来计算健康效果。
基于成本效益和潜在健康结果,扩大规模的最佳途径是从有针对性的 OAE 开始,然后扩大到普遍的 OAE 和普遍的 OAE 加 AABR。筛查、诊断和干预服务的可及性显著影响了方案选择。
总之,为了实现 NHS 计划的成本效益和最佳健康结果,应扩大筛查、诊断和干预服务的可及性,以覆盖更多人群。因此,这些结果有望在国家计划的推广方面带来特别的好处。