Division of Cardiology, St Luke's Roosevelt Hospital, Columbia University College of Physicians and Surgeons, 1000 10th Avenue, New York, NY 10019, USA.
BMJ. 2013 Jan 28;346:f360. doi: 10.1136/bmj.f360.
To compare the long term efficacy and adverse events of dual blockade of the renin-angiotensin system with monotherapy.
Systematic review and meta-analysis.
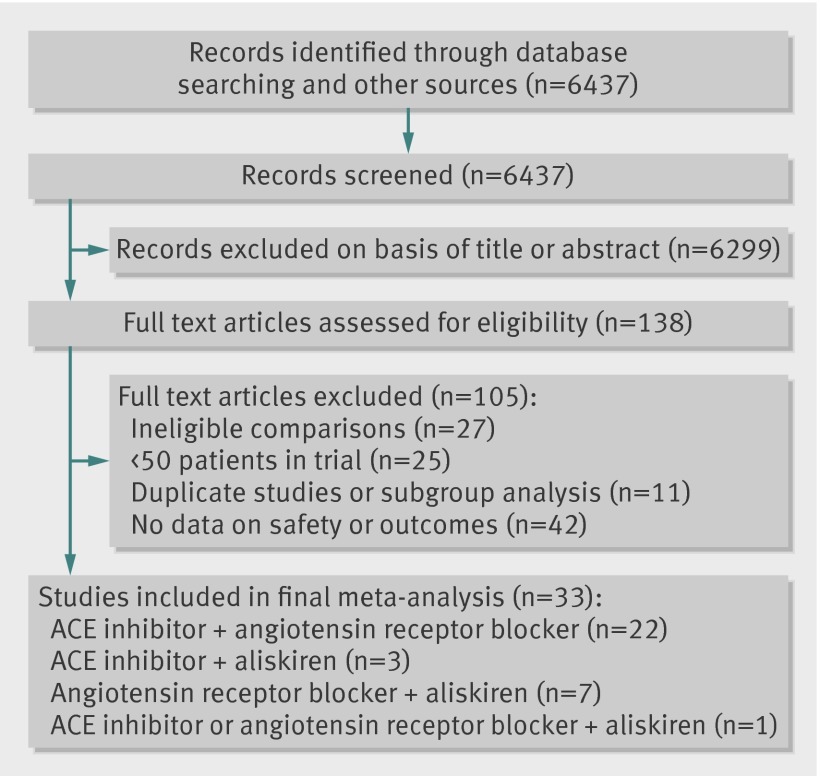
PubMed, Embase, and the Cochrane central register of controlled trials, January 1990 to August 2012.
Randomised controlled trials comparing dual blockers of the renin-angiotensin system with monotherapy, reporting data on either long term efficacy (≥ 1 year) or safety events (≥ 4 weeks), and with a sample size of at least 50. Analysis was stratified by trials with patients with heart failure versus patients without heart failure.
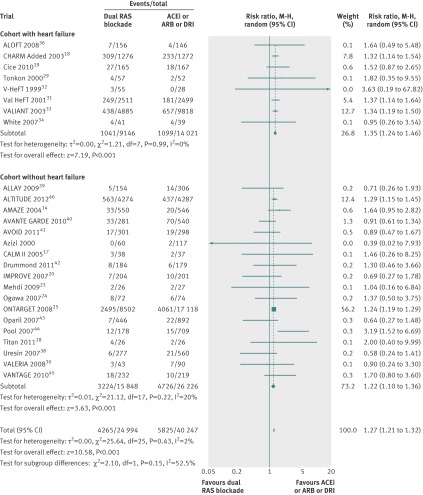
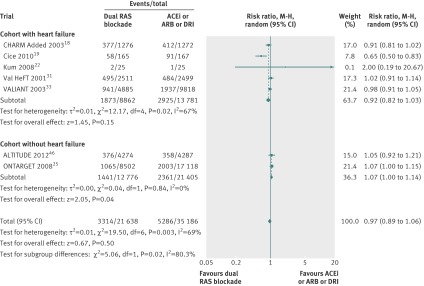
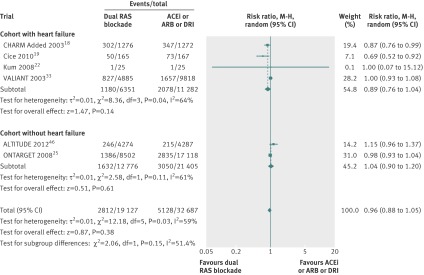
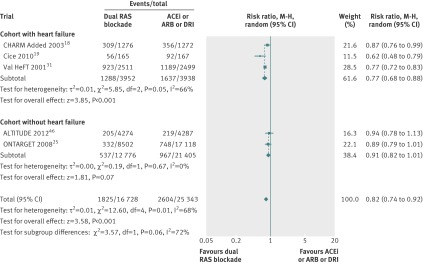
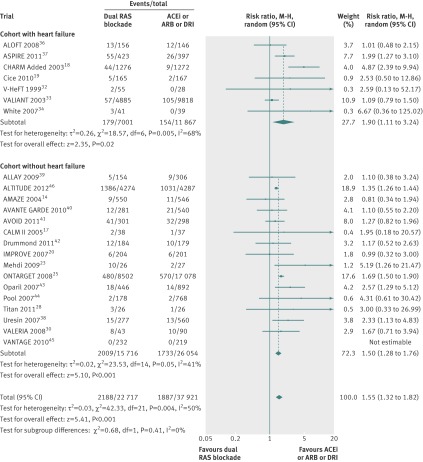
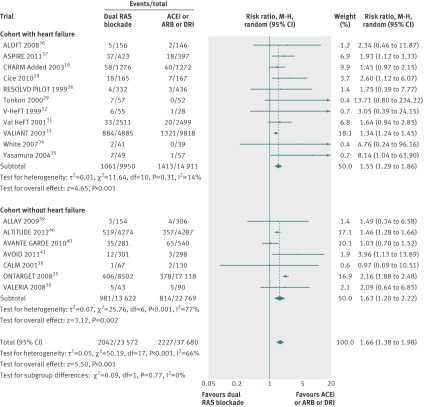
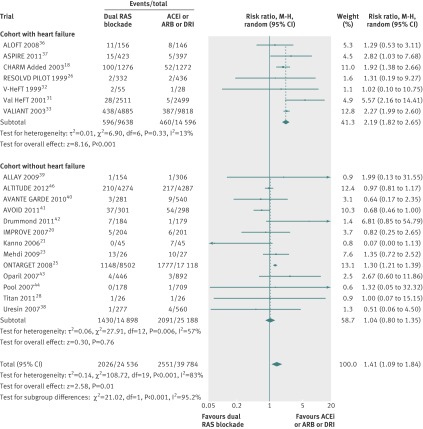
33 randomised controlled trials with 68,405 patients (mean age 61 years, 71% men) and mean duration of 52 weeks were included. Dual blockade of the renin-angiotensin system was not associated with any significant benefit for all cause mortality (relative risk 0.97, 95% confidence interval 0.89 to 1.06) and cardiovascular mortality (0.96, 0.88 to 1.05) compared with monotherapy. Compared with monotherapy, dual therapy was associated with an 18% reduction in admissions to hospital for heart failure (0.82, 0.74 to 0.92). However, compared with monotherapy, dual therapy was associated with a 55% increase in the risk of hyperkalaemia (P<0.001), a 66% increase in the risk of hypotension (P<0.001), a 41% increase in the risk of renal failure (P=0.01), and a 27% increase in the risk of withdrawal owing to adverse events (P<0.001). Efficacy and safety results were consistent in cohorts with and without heart failure when dual therapy was compared with monotherapy except for all cause mortality, which was higher in the cohort without heart failure (P=0.04 v P=0.15), and renal failure was significantly higher in the cohort with heart failure (P<0.001 v P=0.79).
Although dual blockade of the renin-angiotensin system may have seemingly beneficial effects on certain surrogate endpoints, it failed to reduce mortality and was associated with an excessive risk of adverse events such as hyperkalaemia, hypotension, and renal failure compared with monotherapy. The risk to benefit ratio argues against the use of dual therapy.
比较肾素-血管紧张素系统双重阻断与单药治疗的长期疗效和不良事件。
系统评价和荟萃分析。
PubMed、Embase 和 Cochrane 对照试验中心注册库,1990 年 1 月至 2012 年 8 月。
比较肾素-血管紧张素系统双重阻断与单药治疗的随机对照试验,报告长期疗效(≥1 年)或安全性事件(≥4 周)的数据,且样本量至少为 50。根据试验中是否有心衰患者进行分层。
纳入 33 项随机对照试验,共 68405 例患者(平均年龄 61 岁,71%为男性),平均随访时间为 52 周。与单药治疗相比,肾素-血管紧张素系统双重阻断并未显著降低全因死亡率(相对风险 0.97,95%置信区间 0.89 至 1.06)和心血管死亡率(0.96,0.88 至 1.05)。与单药治疗相比,双重治疗可使因心衰住院的风险降低 18%(0.82,0.74 至 0.92)。然而,与单药治疗相比,双重治疗使高钾血症的风险增加 55%(P<0.001),低血压的风险增加 66%(P<0.001),肾衰竭的风险增加 41%(P=0.01),因不良反应停药的风险增加 27%(P<0.001)。当与单药治疗相比时,在有心衰和无心衰的队列中,疗效和安全性结果均一致,除了全因死亡率,在无心衰的队列中更高(P=0.04 比 P=0.15),而在有心衰的队列中,肾衰竭的风险明显更高(P<0.001 比 P=0.79)。
尽管肾素-血管紧张素系统双重阻断可能对某些替代终点有看似有益的影响,但与单药治疗相比,它未能降低死亡率,且与高钾血症、低血压和肾衰竭等不良事件的风险增加相关。风险获益比不利于双重治疗的应用。