MRC/Wits Rural Public Health & Health Transitions Research Unit (Agincourt), School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Glob Health Action. 2013 Jan 24;6:19266. doi: 10.3402/gha.v6i0.19266.
South Africa accounts for more than a sixth of the global population of people infected with HIV and TB, ranking her highest in HIV/TB co-infection worldwide. Remote areas often bear the greatest burden of morbidity and mortality, yet there are spatial differences within rural settings.
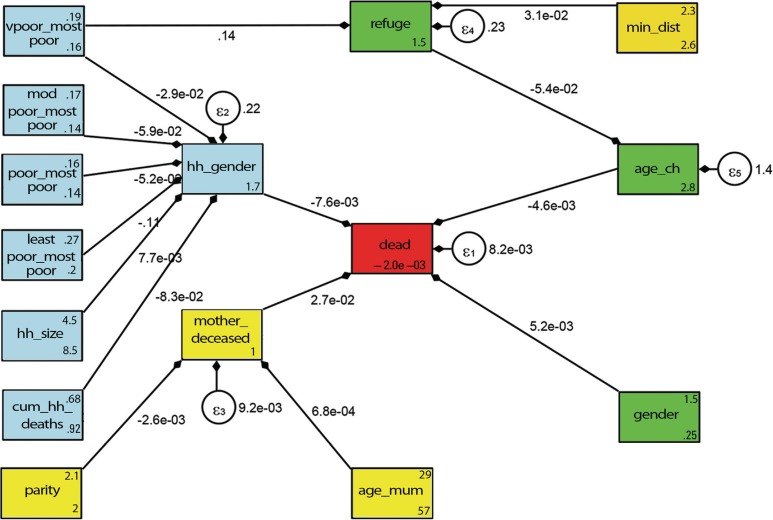
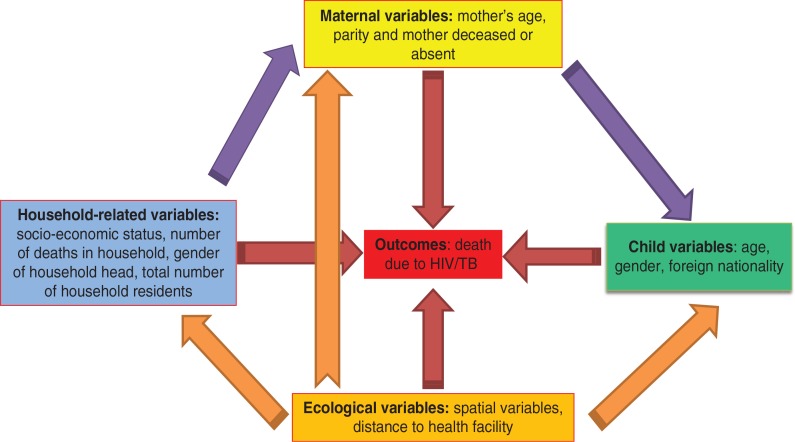
The primary aim was to investigate HIV/TB mortality determinants and their spatial distribution in the rural Agincourt sub-district for children aged 1-5 years in 2004. Our secondary aim was to model how the associated factors were interrelated as either underlying or proximate factors of child mortality using pathway analysis based on a Mosley-Chen conceptual framework.
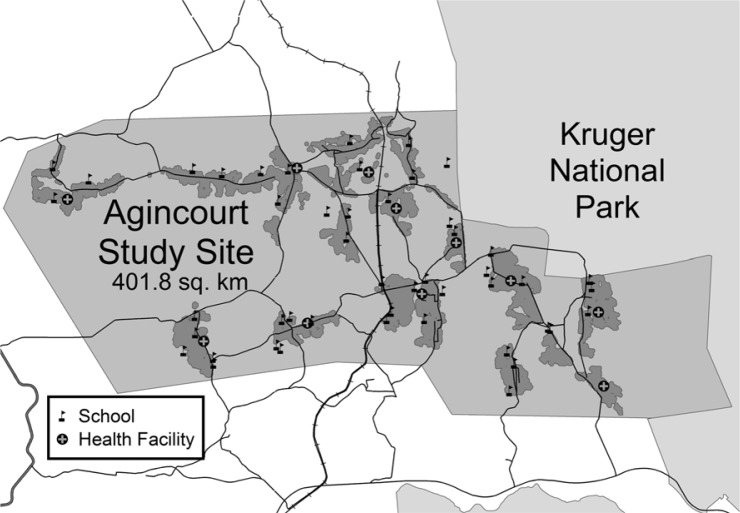
We conducted a secondary data analysis based on cross-sectional data collected in 2004 from the Agincourt sub-district in rural northeast South Africa. Child HIV/TB death was the outcome measure derived from physician assessed verbal autopsy. Modelling used multiple logit regression models with and without spatial household random effects. Structural equation models were used in modelling the complex relationships between multiple exposures and the outcome (child HIV/TB mortality) as relayed on a conceptual framework.
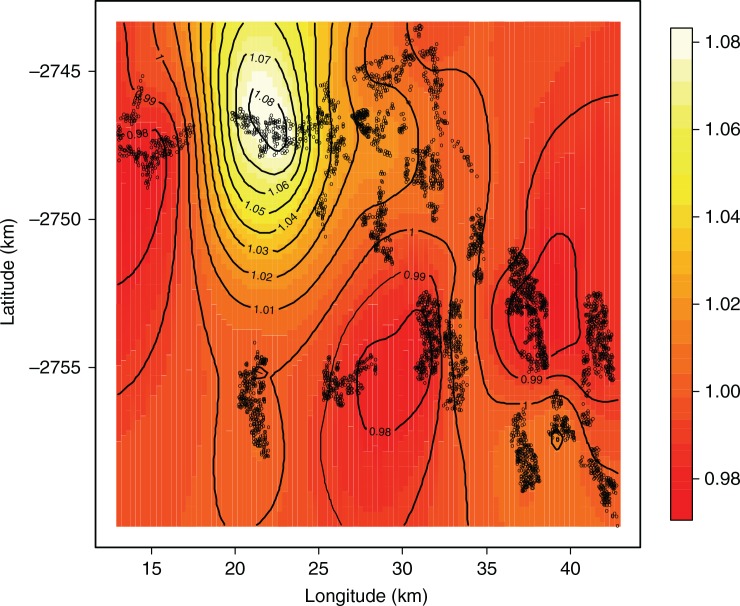
Fifty-four of 6,692 children aged 1-5 years died of HIV/TB, from a total of 5,084 households. Maternal death had the greatest effect on child HIV/TB mortality (adjusted odds ratio=4.00; 95% confidence interval=1.01-15.80). A protective effect was found in households with better socio-economic status and when the child was older. Spatial models disclosed that the areas which experienced the greatest child HIV/TB mortality were those without any health facility.
Low socio-economic status and maternal deaths impacted indirectly and directly on child mortality, respectively. These factors are major concerns locally and should be used in formulating interventions to reduce child mortality. Spatial prediction maps can guide policy makers to target interventions where they are most needed.
南非的艾滋病毒和结核病感染者人数占全球的六分之一以上,是全球艾滋病毒/结核病合并感染率最高的国家。偏远地区往往承受着最大的发病率和死亡率负担,但农村地区也存在空间差异。
本研究的主要目的是调查 2004 年南非农村阿格因库尔茨亚区 1-5 岁儿童艾滋病毒/结核病死亡率的决定因素及其空间分布。我们的次要目的是利用基于 Mosley-Chen 概念框架的路径分析,研究相关因素如何作为儿童死亡的根本或近因因素相互关联。
我们对 2004 年南非东北部农村阿格因库尔茨亚区收集的横断面数据进行了二次数据分析。儿童艾滋病毒/结核病死亡是通过医生评估的口头尸检得出的结果测量指标。模型使用带有和不带有空间家庭随机效应的多项逻辑回归模型进行构建。结构方程模型用于在概念框架下对多个暴露因素与结果(儿童艾滋病毒/结核病死亡率)之间的复杂关系进行建模。
在 6692 名 1-5 岁儿童中,共有 54 名死于艾滋病毒/结核病,来自 5084 个家庭。产妇死亡对儿童艾滋病毒/结核病死亡率的影响最大(调整后的优势比=4.00;95%置信区间=1.01-15.80)。在社会经济地位较好的家庭和孩子年龄较大的家庭中,发现了保护作用。空间模型显示,儿童艾滋病毒/结核病死亡率最高的地区是没有任何卫生设施的地区。
低社会经济地位和产妇死亡分别对儿童死亡率产生间接和直接影响。这些因素是当地的主要关注点,应在制定减少儿童死亡率的干预措施中加以考虑。空间预测图可以指导决策者在最需要的地方进行干预。