Department of Neurosurgery, Oslo University Hospital, Rikshospitalet, and Faculty of Medicine, University of Oslo, Oslo, Norway.
Biomed Eng Online. 2013 Feb 13;12:14. doi: 10.1186/1475-925X-12-14.
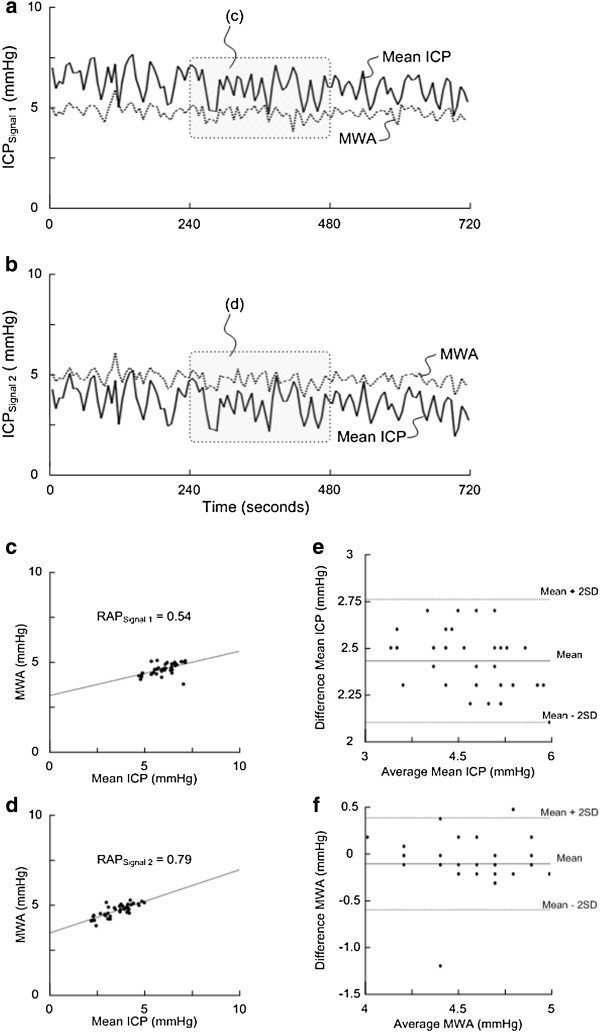
In an attempt to characterize the intracranial pressure-volume compensatory reserve capacity, the correlation coefficient (R) between the ICP wave amplitude (A) and the ICP (P) level (RAP) has been applied in the surveillance of neurosurgical patients. However, as the ICP level may become altered by electrostatic discharges, human factors, technical factors and technology issues related to the ICP sensors, erroneous ICP scores may become revealed to the physician, and also become incorporated into the calculated RAP index. To evaluate the problem with regard to the RAP, we compared simultaneous RAP values from two separate ICP signals in the same patient.
We retrieved our recordings in 20 patients with cerebral bleeds wherein the ICP had been recorded simultaneously from two different sensors. Sensor 1 was always a solid sensor while sensor 2 was a solid sensor (Category A), a fluid sensor (Category B), an air-pouch sensor (Category C), or a fibre-optic sensor (Category D). The simultaneous signals were analyzed with automatic identification of the cardiac induced ICP waves, with subsequent determination and comparison of the Pearson correlation coefficient between mean wave amplitude (MWA) and mean ICP (RAP) for 40 6-s time windows every 4-min period.
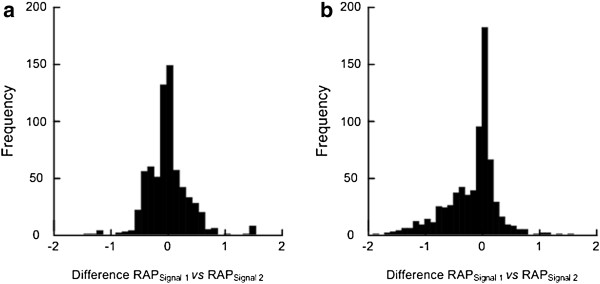
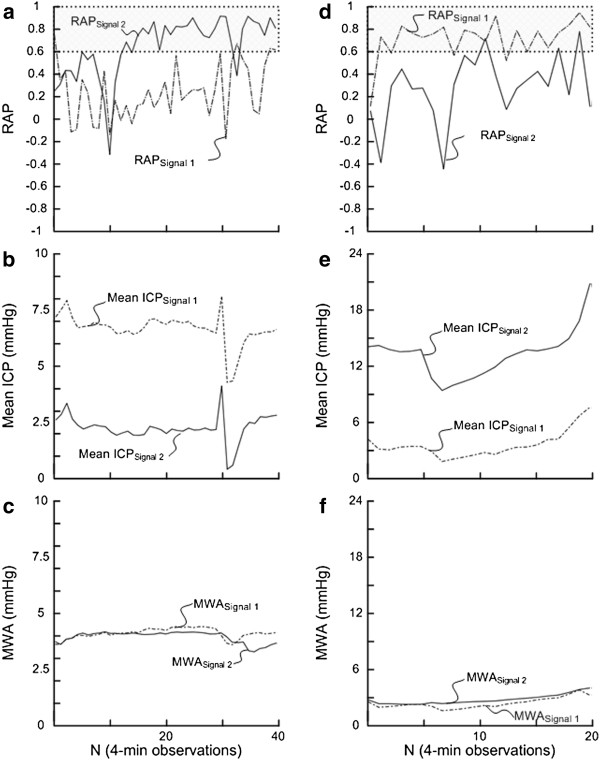
A total of 23,056 4-min RAP observations were compared. A difference in RAP≥0.4 between the two signals was seen in 4% of the observations in Category A-, in 44% of observations in Category B-, in 20% of observations in Category C-, and in 28% of observations in Category D patients, respectively. Moreover, the combination of a RAP of <0.6 in one signal and ≥0.6 in the other was seen in >20% of scores in 3/5 Category A-, in 3/5 Category B-, in 5/7 Category C- and 1/3 Category D patients.
Simultaneous monitoring of the ICP-derived index RAP from two separate ICP sensors reveals marked differences in the index values. These differences in RAP may be explained by erroneous scoring of the ICP level. This will hamper the usefulness of RAP as a guide in the management of neurosurgical patients.
为了描述颅内压-容积补偿储备能力,人们应用颅内压(ICP)波幅(A)与 ICP(P)水平之间的相关系数(R)来监测神经外科患者。然而,由于 ICP 水平可能会受到静电放电、人为因素、技术因素以及与 ICP 传感器相关的技术问题的影响,错误的 ICP 评分可能会被医生发现,并被纳入计算得到的 RAP 指数中。为了评估 RAP 存在的问题,我们比较了同一患者两个独立 ICP 信号的同时 RAP 值。
我们检索了 20 例脑出血患者的记录,这些患者的 ICP 同时由两个不同的传感器记录。传感器 1 始终为固体传感器,而传感器 2 为固体传感器(类别 A)、液体传感器(类别 B)、气袋传感器(类别 C)或光纤传感器(类别 D)。通过自动识别心脏诱导的 ICP 波,对同时的信号进行分析,随后确定并比较每个 4 分钟周期内 40 个 6 秒时间窗的平均波幅(MWA)和平均 ICP(RAP)之间的 Pearson 相关系数。
共比较了 23056 个 4 分钟 RAP 观察值。在类别 A-的观察值中,有 4%的观察值存在两个信号之间的 RAP 差异≥0.4;在类别 B-的观察值中,有 44%的观察值存在差异;在类别 C-的观察值中,有 20%的观察值存在差异;在类别 D-的观察值中,有 28%的观察值存在差异。此外,在 3/5 个类别 A-、3/5 个类别 B-、5/7 个类别 C-和 1/3 个类别 D-患者中,超过 20%的分数中,一个信号的 RAP<0.6,而另一个信号的 RAP≥0.6。
同时监测两个独立的 ICP 传感器得到的 ICP 衍生指数 RAP 显示出指数值的显著差异。这些 RAP 的差异可能是由于 ICP 水平的错误评分所致。这将妨碍 RAP 作为指导神经外科患者管理的有用性。