Screening and Test Evaluation Program, School of Public Health, University of Sydney, Sydney 2006, Australia.
BMJ. 2013 Feb 13;346:f866. doi: 10.1136/bmj.f866.
To determine the accuracy of a clinical decision rule (the traffic light system developed by the National Institute for Health and Clinical Excellence (NICE)) for detecting three common serious bacterial infections (urinary tract infection, pneumonia, and bacteraemia) in young febrile children.
Retrospective analysis of data from a two year prospective cohort study
A paediatric emergency department.
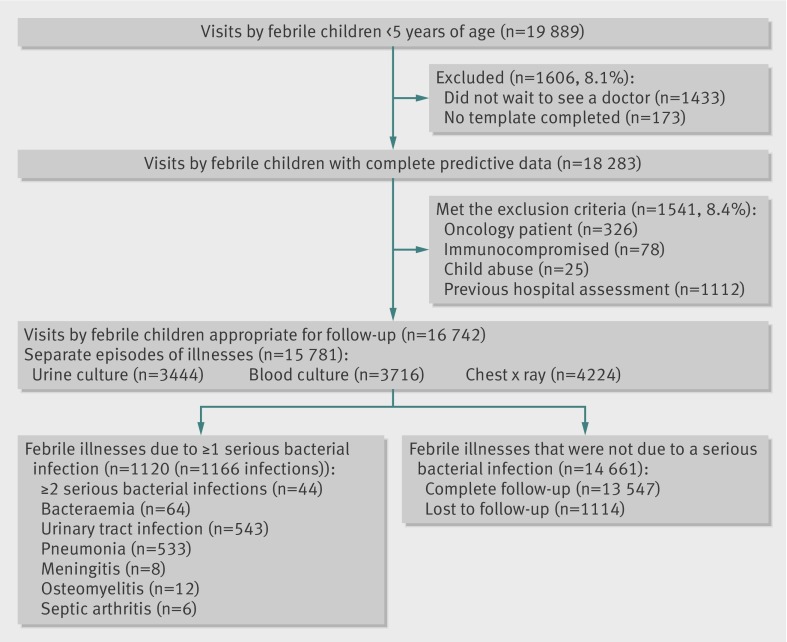
15,781 cases of children under 5 years of age presenting with a febrile illness.
Clinical features were used to categorise each febrile episodes as low, intermediate, or high probability of serious bacterial infection (green, amber, and red zones of the traffic light system); these results were checked (using standard radiological and microbiological tests) for each of the infections of interest and for any serious bacterial infection.
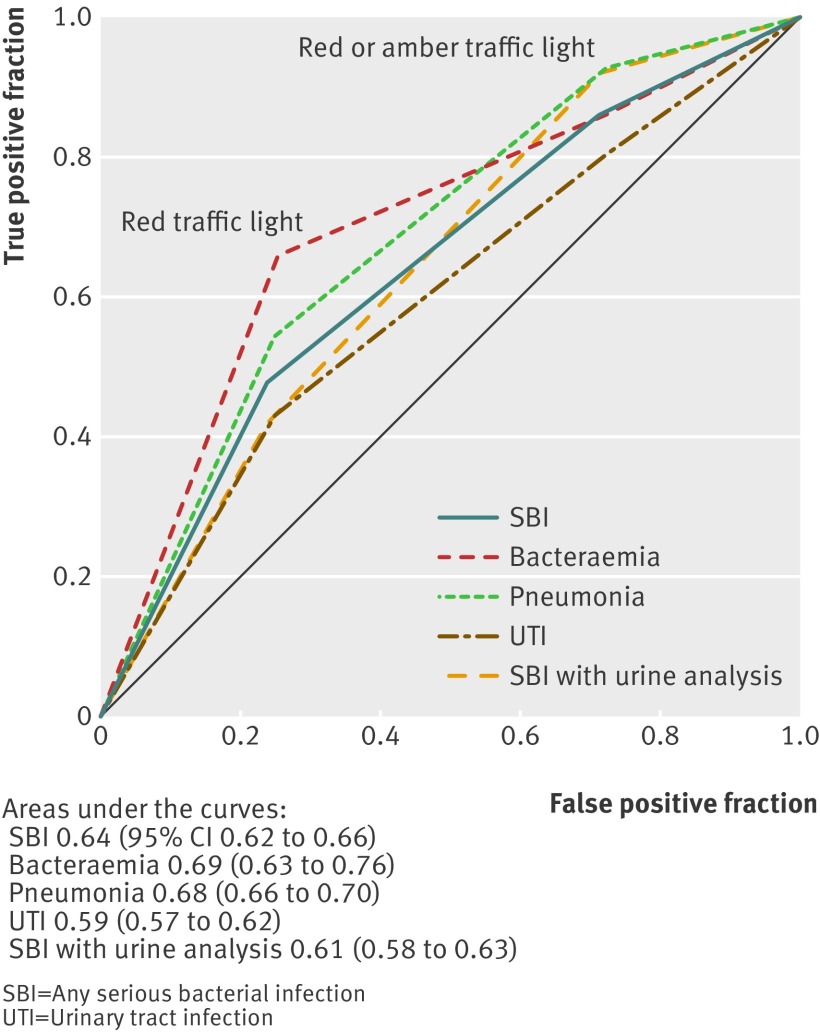
After combination of the intermediate and high risk categories, the NICE traffic light system had a test sensitivity of 85.8% (95% confidence interval 83.6% to 87.7%) and specificity of 28.5% (27.8% to 29.3%) for the detection of any serious bacterial infection. Of the 1140 cases of serious bacterial infection, 157 (13.8%) were test negative (in the green zone), and, of these, 108 (68.8%) were urinary tract infections. Adding urine analysis (leucocyte esterase or nitrite positive), reported in 3653 (23.1%) episodes, to the traffic light system improved the test performance: sensitivity 92.1% (89.3% to 94.1%), specificity 22.3% (20.9% to 23.8%), and relative positive likelihood ratio 1.10 (1.06 to 1.14).
The NICE traffic light system failed to identify a substantial proportion of serious bacterial infections, particularly urinary tract infections. The addition of urine analysis significantly improved test sensitivity, making the traffic light system a more useful triage tool for the detection of serious bacterial infections in young febrile children.
确定国家卫生与临床优化研究所(NICE)开发的临床决策规则(红绿灯系统)用于检测年轻发热儿童三种常见严重细菌感染(尿路感染、肺炎和菌血症)的准确性。
对一项为期两年的前瞻性队列研究数据的回顾性分析。
儿科急诊室。
15781 例 5 岁以下发热儿童。
临床特征用于将每个发热病例分类为低、中、高严重细菌感染概率(红绿灯系统的绿、黄、红区);对于所有感兴趣的感染和任何严重细菌感染,都检查了这些结果(使用标准放射学和微生物学检查)。
将中间风险和高风险类别合并后,NICE 红绿灯系统检测任何严重细菌感染的敏感度为 85.8%(95%置信区间 83.6%至 87.7%),特异性为 28.5%(27.8%至 29.3%)。在 1140 例严重细菌感染中,有 157 例(13.8%)检测结果为阴性(在绿区),其中 108 例(68.8%)为尿路感染。将红绿灯系统中报告的 3653 例(23.1%)尿液分析(白细胞酯酶或亚硝酸盐阳性)纳入其中,提高了检测性能:敏感度 92.1%(89.3%至 94.1%),特异性 22.3%(20.9%至 23.8%),相对阳性似然比 1.10(1.06 至 1.14)。
NICE 红绿灯系统未能识别出相当一部分严重细菌感染,尤其是尿路感染。添加尿液分析显著提高了检测敏感度,使红绿灯系统成为检测年轻发热儿童严重细菌感染更有用的分诊工具。