Haemophilia and Thrombosis Centre, University Hospital of Wales, , Cardiff, UK.
Emerg Med J. 2014 Feb;31(2):163-8. doi: 10.1136/emermed-2012-201976. Epub 2013 Feb 22.
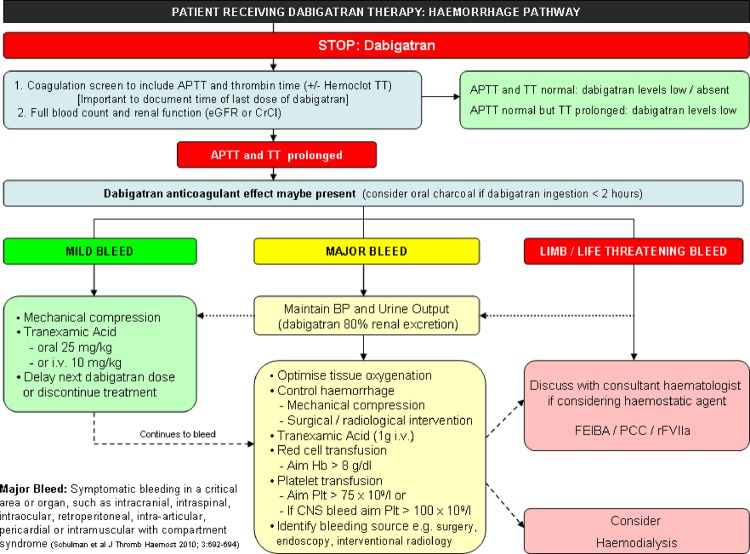
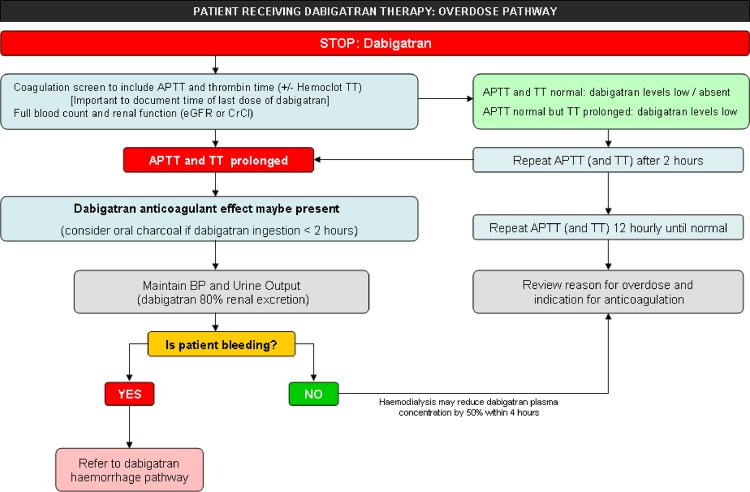
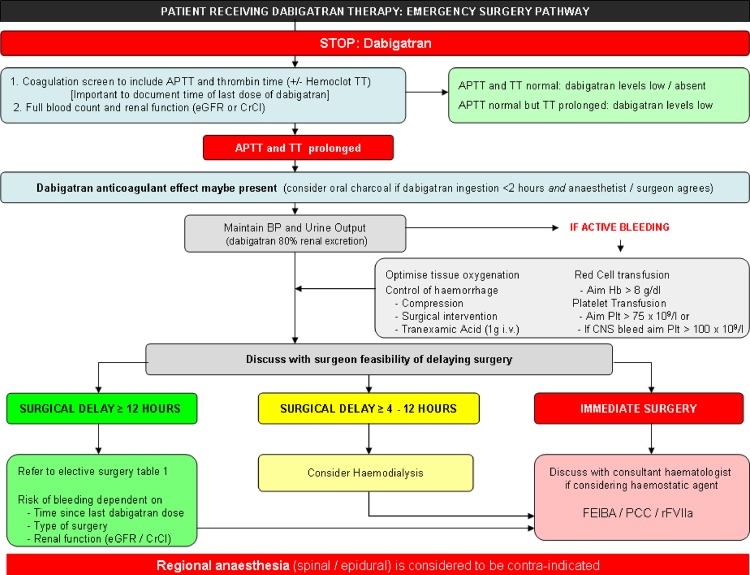
Dabigatran is an oral direct thrombin inhibitor (DTI) licensed for stroke prevention in atrial fibrillation and likely to be soon approved in Europe for treatment of venous thrombosis. Predictable pharmacokinetics and a reduced risk of intracranial haemorrhage do not negate the potential risk of haemorrhage. Unlike warfarin, there is no reversal agent and measurement of the anticoagulant effect is not 'routine'. The prothrombin time/international normalised ratio response to dabigatran is inconsistent and should not be measured when assessing a patient who is bleeding or needs emergency surgery. The activated partial thromboplastin time (APTT) provides a qualitative measurement of the anticoagulant effect of dabigatran. Knowledge of the time of last dose is important for interpretation of the APTT. Commercially available DTI assays provide a quantitative measurement of active dabigatran concentration in the plasma. If a patient receiving dabigatran presents with bleeding: omit/delay next dose of dabigatran; measure APTT and thrombin time (consider DTI assay if available); administer activated charcoal, with sorbitol, if within 2 h of dabigatran ingestion; give tranexamic acid (1 g intravenously if significant bleeding); maintain renal perfusion and urine output to aid dabigatran excretion. Dabigatran exhibits low protein binding and may be removed by dialysis. Supportive care should form the mainstay of treatment. If bleeding is life/limb threatening, consider an additional haemostatic agent. There is currently no evidence to support the choice of one haemostatic agent (FEIBA, recombinant factor VIIa, prothrombin complex concentrates) over another. Choice will depend on access to and experience with available haemostatic agent(s).
达比加群酯是一种口服直接凝血酶抑制剂(DTI),已获许可用于预防房颤患者发生中风,并且可能很快在欧洲获准用于治疗静脉血栓形成。可预测的药代动力学和降低颅内出血的风险并不能消除出血的潜在风险。与华法林不同,它没有逆转剂,且抗凝效果的检测并非“常规”。达比加群酯对凝血酶原时间/国际标准化比值的反应不一致,在评估正在出血或需要紧急手术的患者时,不应进行检测。激活部分凝血活酶时间(APTT)可定性检测达比加群酯的抗凝效果。了解最后一次给药的时间对于 APTT 的解读非常重要。市售的 DTI 检测可提供血浆中达比加群酯的活性浓度的定量测量。如果正在接受达比加群酯治疗的患者出现出血:停用/延迟下一次达比加群酯给药;测量 APTT 和凝血酶时间(如果有条件,考虑 DTI 检测);如果在达比加群酯摄入后 2 小时内,给予活性炭和山梨醇;给予氨甲环酸(如果有明显出血,静脉内给予 1 g);维持肾脏灌注和尿量,以促进达比加群酯的排泄。达比加群酯的蛋白结合率低,可能通过透析清除。支持性治疗应是治疗的主要方法。如果出血危及生命/肢体,考虑使用其他止血剂。目前尚无证据支持选择一种止血剂(FEIBA、重组凝血因子 VIIa、凝血酶原复合物浓缩物)优于另一种。选择将取决于可获得的止血剂和使用经验。