The Johns Hopkins Hospital, Meyer 8-154, Baltimore, MD 21287, USA.
Stroke. 2013 Apr;44(4):1158-61. doi: 10.1161/STROKEAHA.111.000033. Epub 2013 Mar 5.
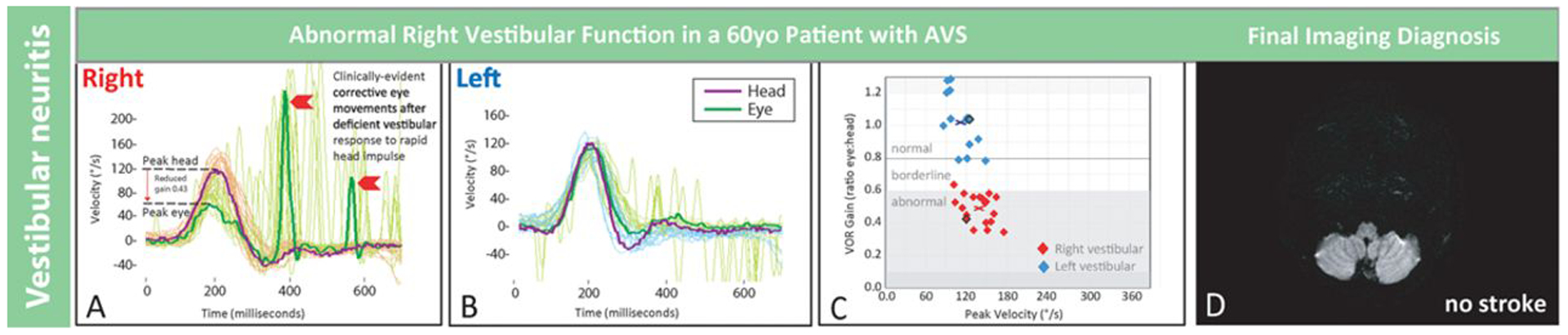
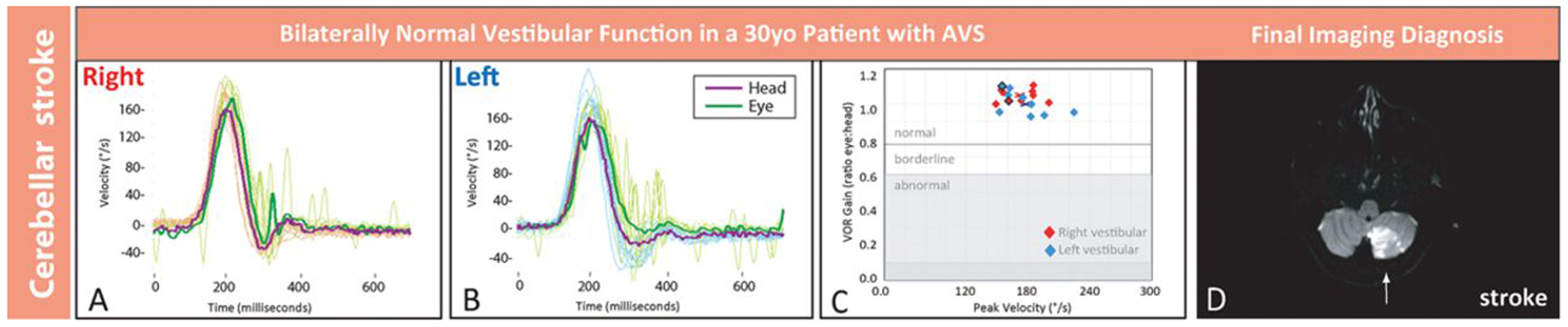
Strokes can be distinguished from benign peripheral causes of acute vestibular syndrome using bedside oculomotor tests (head impulse test, nystagmus, test-of-skew). Using head impulse test, nystagmus, test-of-skew is more sensitive and less costly than early magnetic resonance imaging for stroke diagnosis in acute vestibular syndrome but requires expertise not routinely available in emergency departments. We sought to begin standardizing the head impulse test, nystagmus, test-of-skew diagnostic approach for eventual emergency department use through the novel application of a portable video-oculography device measuring vestibular physiology in real time. This approach is conceptually similar to ECG to diagnose acute cardiac ischemia.
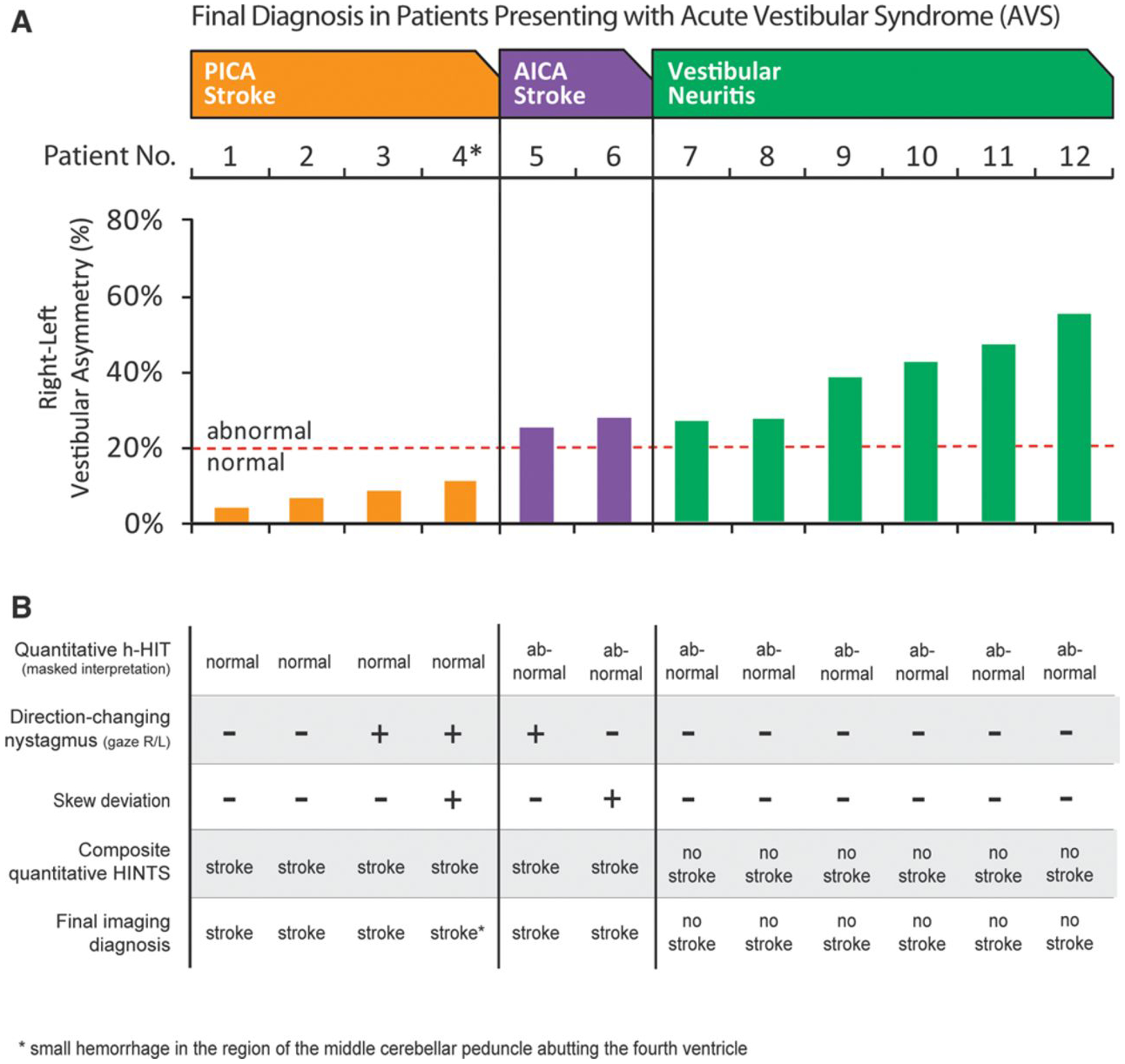
Proof-of-concept study (August 2011 to June 2012). We recruited adult emergency department patients with acute vestibular syndrome defined as new, persistent vertigo/dizziness, nystagmus, and (1) nausea/vomiting, (2) head motion intolerance, or (3) new gait unsteadiness. We recorded eye movements, including quantitative horizontal head impulse testing of vestibulo-ocular-reflex function. Two masked vestibular experts rated vestibular findings, which were compared with final radiographic gold-standard diagnoses. Masked neuroimaging raters determined stroke or no stroke using magnetic resonance imaging of the brain with diffusion-weighted imaging obtained 48 hours to 7 days after symptom onset.
We enrolled 12 consecutive patients who underwent confirmatory magnetic resonance imaging. Mean age was 61 years (range 30-73), and 10 were men. Expert-rated video-oculography-based head impulse test, nystagmus, test-of-skew examination was 100% accurate (6 strokes, 6 peripheral vestibular).
Device-based physiological diagnosis of vertebrobasilar stroke in acute vestibular syndrome should soon be possible. If confirmed in a larger sample, this bedside eye ECG approach could eventually help fulfill a critical need for timely, accurate, efficient diagnosis in emergency department patients with vertigo or dizziness who are at high risk for stroke.
使用床边眼动测试(摇头试验、眼震、偏斜试验)可将中风与良性外周性急性前庭综合征相区分。与早期磁共振成像(MRI)相比,使用摇头试验、眼震、偏斜试验诊断急性前庭综合征中的中风具有更高的敏感性和更低的成本,但需要在急诊中不常具备的专业知识。我们试图通过新颖的应用便携式视频眼动描记术实时测量前庭生理学,开始使摇头试验、眼震、偏斜试验诊断方法标准化,以便最终应用于急诊。这种方法在概念上类似于用于诊断急性心肌缺血的心电图。
概念验证研究(2011 年 8 月至 2012 年 6 月)。我们招募了有急性前庭综合征的成年急诊患者,该综合征定义为新发、持续性眩晕/头晕、眼震,且(1)恶心/呕吐,(2)头部运动不耐受,或(3)新发步态不稳。我们记录了眼球运动,包括前庭眼反射功能的定量水平摇头测试。两位盲法前庭专家对前庭发现进行评分,并将其与最终影像学金标准诊断进行比较。盲法神经影像学评分者使用发病后 48 小时至 7 天的头部 MRI 加弥散加权成像来确定是否为中风。
我们纳入了 12 例连续接受确认性 MRI 的患者。平均年龄为 61 岁(范围 30-73 岁),10 例为男性。基于视频眼动描记术的摇头试验、眼震、偏斜试验的专家评分准确率为 100%(6 例中风,6 例周围性前庭)。
急性前庭综合征中椎基底动脉性中风的基于设备的生理学诊断应该很快成为可能。如果在更大的样本中得到证实,这种床边眼心电图方法最终可能有助于满足急诊中头晕或眩晕且中风风险高的患者对及时、准确、有效的诊断的迫切需求。