Scott Megan, Mehta Sonia, Rahman Hassan T, Grossniklaus Hans E, Yeh Steven
Division of Vitreoretinal Surgery and Disease, Department of Ophthalmology, Emory University School of Medicine, Atlanta, GA, USA.
J Ophthalmic Inflamm Infect. 2013 Mar 30;3(1):44. doi: 10.1186/1869-5760-3-44.
Endogenous endophthalmitis secondary to Nocardia species is extremely rare but often portends a poor visual prognosis often owing to the advanced nature of disease at presentation and delay in diagnosis. Patients who are systemically immunosuppressed are at greatest risk and early suspicion of the role of this organism in patients with acute panuveitis is paramount.
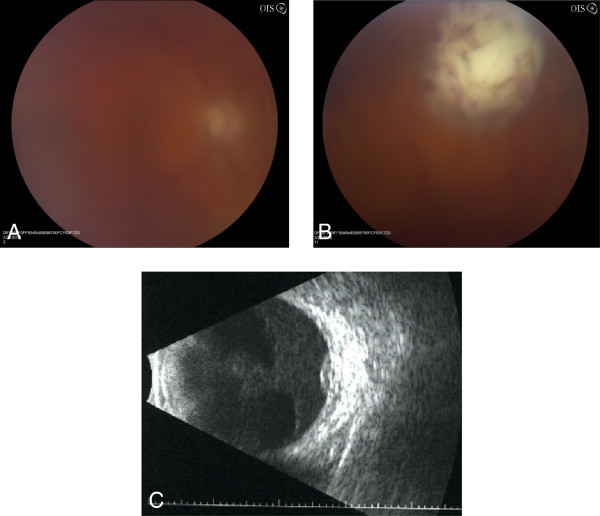
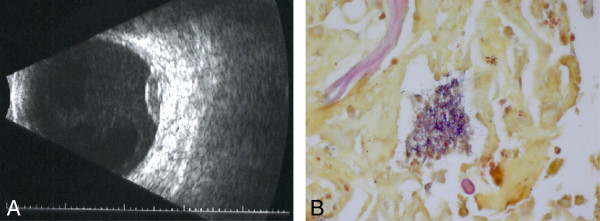
A 66-year-old cardiac transplant patient on oral prednisone, Myfortic, and tacrolimus developed unilateral panuveitis with a focal white subretinal and retinal lesion. His past medical history was notable for Aspergillus pneumonia and cytomegalovirus retinitis in the contralateral eye 12 months prior. Aqueous humor sampling for eubacterial, eufungal, and viral PCR testing, as well as vitreous cultures for bacteria and fungi were unsuccessful in the identification of a causative organism. Progressive enlargement of the lesion was noted despite intravitreal foscarnet, vancomycin, ceftazidime, and voriconazole. A pars plana vitrectomy and retinal and subretinal biopsy led to the identification of Nocardia veterana, a recently identified Nocardia species. A combination of linezolid, meropenem, azithromycin, ceftriaxone, and intravitreal amikacin resulted in eradication of the infection.
This is the first reported case of N. veterana endogenous endophthalmitis in an immunosuppressed patient. Pars plana vitrectomy with a subretinal biopsy was required to establish a diagnosis, as other testing including aqueous PCR and vitreous cultures were negative. The poor visual outcome in our patient highlights the importance of early consideration of Nocardia in the differential diagnosis of panuveitis with subretinal disease in the context of immunosuppression.
由诺卡菌属引起的内源性眼内炎极为罕见,但由于疾病在就诊时已处于晚期且诊断延迟,往往预示着视力预后不良。全身免疫抑制的患者风险最大,早期怀疑该病原体在急性全葡萄膜炎患者中的作用至关重要。
一名66岁的心脏移植患者,正在口服泼尼松、米芙(Myfortic)和他克莫司,出现了单侧全葡萄膜炎,并伴有局灶性白色视网膜下和视网膜病变。他的既往病史值得注意的是,12个月前对侧眼曾患曲霉菌性肺炎和巨细胞病毒性视网膜炎。对房水进行真细菌、真真菌和病毒PCR检测,以及对玻璃体进行细菌和真菌培养,均未能鉴定出致病病原体。尽管给予玻璃体内膦甲酸、万古霉素、头孢他啶和伏立康唑治疗,病变仍逐渐扩大。经扁平部玻璃体切除术及视网膜和视网膜下活检,鉴定出诺卡菌属的新星诺卡菌,这是一种最近才被鉴定出的诺卡菌。利奈唑胺、美罗培南、阿奇霉素、头孢曲松和玻璃体内阿米卡星联合使用,使感染得以根除。
这是免疫抑制患者中首例新星诺卡菌引起的内源性眼内炎的报道病例。由于包括房水PCR和玻璃体培养在内的其他检测均为阴性,因此需要进行扁平部玻璃体切除术及视网膜下活检以确诊。我们患者的不良视力结果凸显了在免疫抑制背景下,对全葡萄膜炎伴视网膜下疾病进行鉴别诊断时,早期考虑诺卡菌的重要性。