Rajagopala Srinivas, Singh Navneet, Agarwal Ritesh, Gupta Dheeraj, Das Reena
Department of Pulmonology and Critical Care, Global Hospitals and Health City, Chennai, India.
Indian J Crit Care Med. 2012 Oct;16(4):198-203. doi: 10.4103/0972-5229.106501.
Hemophagocytic lymphohistiocytosis (HLH) has been reported to complicate fulminant tropical infections but data on severe HLH with multi-organ dysfunction (MODS) are scant.
Retrospective review of medical electronic records of our intensive care unit (ICU) over a 2-year period.
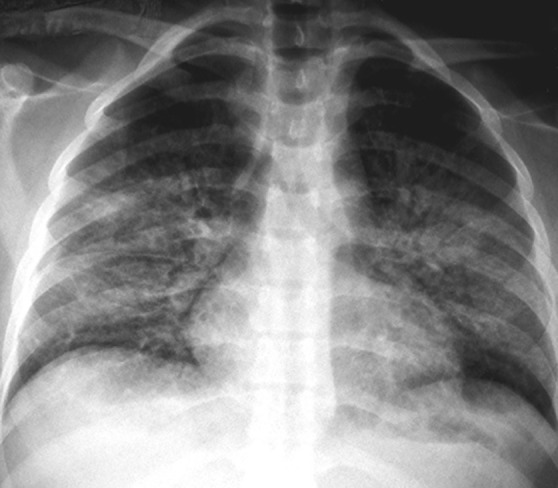
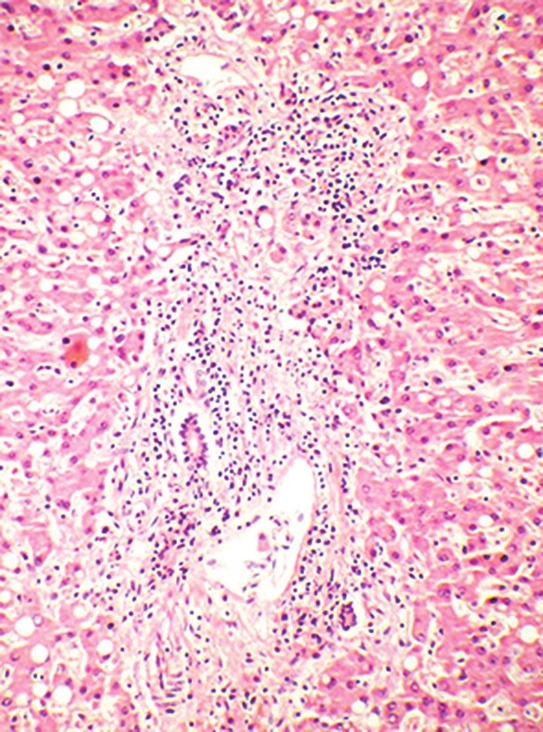
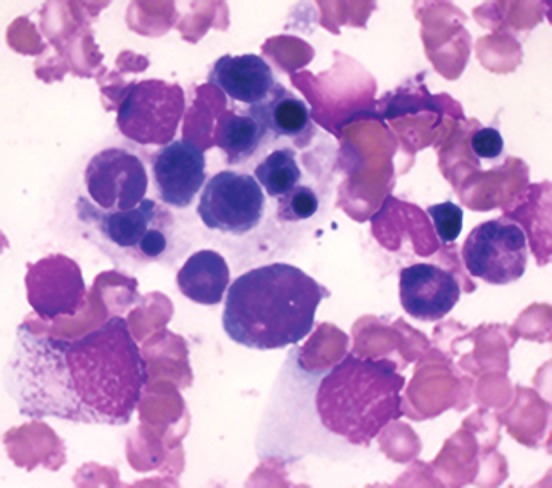
We describe 10 adult patients with HLH and MODS. Patients had short symptom duration prior to presentation and had rapid deterioration during their hospitalization course. Fever, organomegaly, neurologic abnormalities, hepatic abnormalities, and cutaneous signs were very common. No patient had diagnosed HLH at ICU admission (median 4 criteria [Inter Quartile Range 2-4.25]). All patients required mechanical ventilation and 80% required vasopressors. Infection-associated HLH (IAHS) was the most common etiology (80%). Seventy percent (7/10) of patients were treated with steroids and 20% received intravenous immunoglobulin. Etoposide and/or cyclosporine were administered in 20% (2/10). Nosocomial infections occurred in 40% and the ICU mortality was 70%.
Severe HLH with MODS has a very high mortality. Data on adult cohorts with IAHS in the tropics with defined treatment protocols are urgently needed.
噬血细胞性淋巴组织细胞增生症(HLH)已被报道可并发暴发性热带感染,但关于伴有多器官功能障碍(MODS)的严重HLH的数据却很少。
回顾性分析我们重症监护病房(ICU)两年期间的医疗电子记录。
我们描述了10例患有HLH和MODS的成年患者。患者在就诊前症状持续时间短,住院期间病情迅速恶化。发热、器官肿大、神经异常、肝脏异常和皮肤体征非常常见。在ICU入院时,没有患者被诊断为HLH(中位数为4项标准[四分位间距2 - 4.25])。所有患者均需要机械通气,80%的患者需要血管活性药物。感染相关的HLH(IAHS)是最常见的病因(80%)。70%(7/10)的患者接受了类固醇治疗,20%的患者接受了静脉注射免疫球蛋白治疗。20%(2/10)的患者使用了依托泊苷和/或环孢素。医院感染发生率为40%,ICU死亡率为70%。
伴有MODS的严重HLH死亡率非常高。迫切需要有关热带地区具有明确治疗方案的IAHS成年队列的数据。