School of Nursing and Midwifery, University of Western Sydney, Penrith South DC, NSW, Australia.
BMC Pregnancy Childbirth. 2013 Apr 8;13:89. doi: 10.1186/1471-2393-13-89.
Severe perineal trauma occurs in 0.5-10% of vaginal births and can result in significant morbidity including pain, dyspareunia and faecal incontinence. The aim of this study is to determine the risk of recurrence, subsequent mode of birth and morbidity for women who experienced severe perineal trauma during their first birth in New South Wales (NSW) between 2000 - 2008.
All singleton births recorded in the NSW Midwives Data Collection between 2000-2008 (n=510,006) linked to Admitted Patient Data were analysed. Determination of morbidity was based upon readmission to hospital within a 12 month time period following birth for a surgical procedure falling within four categories: 1. Vaginal repair, 2. Fistula repair, 3. Faecal and urinary incontinence repair, and 4. Rectal/anal repair. Women who experienced severe perineal trauma during their first birth were compared to women who did not.
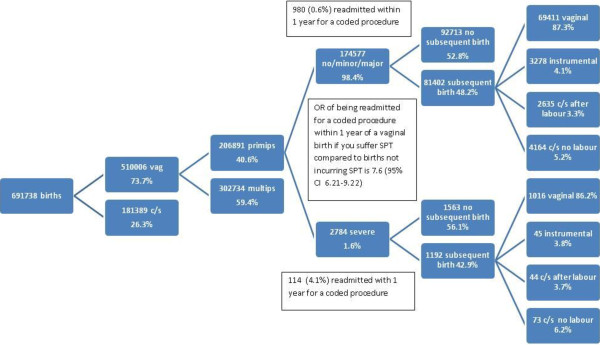
2,784 (1.6%) primiparous women experienced severe perineal trauma during this period. Primiparous women experiencing severe perineal trauma were less likely to have a subsequent birth (56% vs 53%) compared to those not who did not (OR 0.9; CI 0.81-0.99), however there was no difference in the subsequent rate of elective caesarean section (OR 1.2; 0.95-1.54), vaginal birth (including instrumental birth) (OR 1.0; CI 0.81-1.17) or normal vaginal birth (excluding instrumental birth) (OR 1.0; CI 0.85-1.17). Women were no more likely to have a severe perineal tear in the second birth if they experienced this in the first (OR 0.9; CI 0.67-1.34). Women who had a severe perineal tear in their first birth were significantly more likely to have an 'associated surgical procedure' within the ≤12 months following birth (vaginal repair following primary repair, rectal/anal repair following primary repair, fistula repair and urinary/faecal incontinence repair) (OR 7.6; CI 6.21-9.22). Women who gave birth in a private hospital compared to a public hospital were more likely to have an 'associated surgical procedure' in the 12 months following the birth (OR 1.8; CI 1.54-1.97), regardless of parity, birth type and perineal status.
Primiparous women who experience severe perineal trauma are less likely to have a subsequent baby, more likely to have a related surgical procedure in the 12 months following the birth and no more likely to have an operative birth or another severe perineal tear in a subsequent birth. Women giving birth in a private hospital are more likely to have an associated surgical procedure in the 12 months following birth.
严重的会阴创伤发生在 0.5-10%的阴道分娩中,可导致显著的发病率,包括疼痛、性交困难和粪便失禁。本研究的目的是确定在新南威尔士州(NSW)2000-2008 年间首次分娩中经历严重会阴创伤的妇女在随后的妊娠中复发、分娩方式和发病率的风险。
对 2000-2008 年间 NSW 助产士数据收集(n=510,006)中记录的所有单胎分娩进行分析,并与住院患者数据相关联。发病率的确定是基于分娩后 12 个月内因四类手术之一而再次住院:1. 阴道修复,2. 瘘管修复,3. 粪便和尿失禁修复,4. 直肠/肛门修复。与未经历严重会阴创伤的产妇相比,首次分娩中经历严重会阴创伤的产妇。
在此期间,2784 名(1.6%)初产妇经历了严重的会阴创伤。与未经历严重会阴创伤的产妇相比,经历严重会阴创伤的初产妇随后的分娩率较低(56%对 53%)(OR 0.9;95%CI 0.81-0.99),但随后的选择性剖宫产率(OR 1.2;95%CI 0.95-1.54)、阴道分娩(包括器械分娩)(OR 1.0;95%CI 0.81-1.17)或正常阴道分娩(不包括器械分娩)(OR 1.0;95%CI 0.85-1.17)无差异。如果产妇在第一次分娩中经历了严重的会阴撕裂,那么她们在第二次分娩中发生严重会阴撕裂的可能性也不会增加(OR 0.9;95%CI 0.67-1.34)。在第一次分娩中经历了严重会阴撕裂的产妇在分娩后 12 个月内更有可能进行“相关手术”(初次修复后的阴道修复、初次修复后的直肠/肛门修复、瘘管修复以及尿/粪便失禁修复)(OR 7.6;95%CI 6.21-9.22)。与公立医院相比,在私立医院分娩的产妇在分娩后 12 个月内更有可能进行“相关手术”(OR 1.8;95%CI 1.54-1.97),无论其产次、分娩类型和会阴状况如何。
经历严重会阴创伤的初产妇随后生育的可能性较低,在分娩后 12 个月内更有可能进行相关手术,在随后的分娩中再次发生阴道分娩或另一次严重会阴撕裂的可能性也较低。在私立医院分娩的产妇在分娩后 12 个月内更有可能进行相关手术。