Department of Psychiatry, Chang-Gung Memorial Hospital at Linkou and Chang-Gung University School of Medicine, Taoyuan, Taiwan.
J Headache Pain. 2013 Feb 27;14(1):19. doi: 10.1186/1129-2377-14-19.
No study has been performed to compare the impacts of migraine and major depressive episode (MDE) on depression, anxiety and somatic symptoms, and health-related quality of life (HRQoL) among psychiatric outpatients. The aim of this study was to investigate the above issue.
This study enrolled consecutive psychiatric outpatients with mood and/or anxiety disorders who undertook a first visit to a medical center. Migraine was diagnosed according to the International Classification of Headache Disorders, 2nd edition. Three psychometric scales and the Short-Form 36 were administered. General linear models were used to estimate the difference in scores contributed by either migraine or MDE. Multiple linear regressions were employed to compare the variance of these scores explained by migraine or MDE.
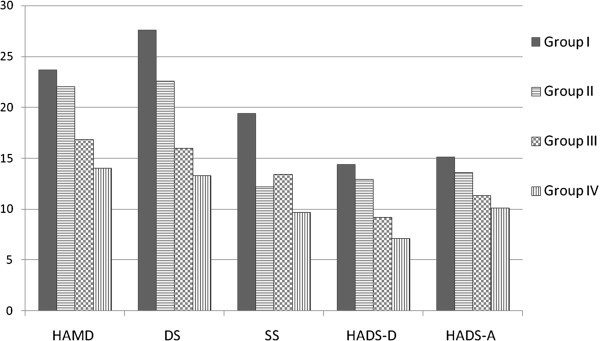
Among 214 enrolled participants, 35.0% had migraine. Bipolar II disorder patients (70.0%) had the highest percentage of migraine, followed by major depressive disorder (49.1%) and only anxiety disorder (24.5%). Patients with migraine had worse depression, anxiety, and somatic symptoms and lower SF-36 scores than those without. The estimated differences in the scores of physical functioning, bodily pain, and somatic symptoms contributed by migraine were not lower than those contributed by MDE. The regression model demonstrated the variance explained by migraine was significantly greater than that explained by MDE in physical and pain symptoms.
Migraine was common and the impact of migraine on physical and pain symptoms was greater than MDE among psychiatric outpatients. Integration of treatment strategies for migraine into psychiatric treatment plans should be considered.
目前尚无研究比较偏头痛和重性抑郁发作(MDE)对精神科门诊患者的抑郁、焦虑和躯体症状以及健康相关生活质量(HRQoL)的影响。本研究旨在探讨这一问题。
本研究纳入了首次就诊于医疗中心的伴有心境或焦虑障碍的连续精神科门诊患者。偏头痛的诊断依据为《国际头痛疾病分类》第 2 版。采用 3 种心理计量学量表和简明健康状况量表(SF-36)进行评估。采用一般线性模型估计偏头痛或 MDE 对评分的差异贡献。采用多元线性回归比较偏头痛或 MDE 对这些评分的方差解释。
在纳入的 214 名患者中,35.0%有偏头痛。双相 II 型障碍患者(70.0%)偏头痛的比例最高,其次是重性抑郁障碍(49.1%)和仅有焦虑障碍(24.5%)。偏头痛患者的抑郁、焦虑和躯体症状更严重,SF-36 评分更低。偏头痛对生理功能、身体疼痛和躯体症状评分的影响估计差异并不低于 MDE。回归模型表明,偏头痛在生理和疼痛症状方面解释的方差明显大于 MDE。
偏头痛在精神科门诊患者中较为常见,偏头痛对躯体症状的影响大于 MDE。应考虑将偏头痛的治疗策略整合到精神科治疗计划中。