Radiation Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, National Institutes of Health, Bethesda, Maryland 20892, USA.
Int J Radiat Oncol Biol Phys. 2013 Jul 15;86(4):694-701. doi: 10.1016/j.ijrobp.2013.03.014. Epub 2013 Apr 26.
To provide dosimetric data for an epidemiologic study on the risk of second primary esophageal cancer among breast cancer survivors, by reconstructing the radiation dose incidentally delivered to the esophagus of 414 women treated with radiation therapy for breast cancer during 1943-1996 in North America and Europe.
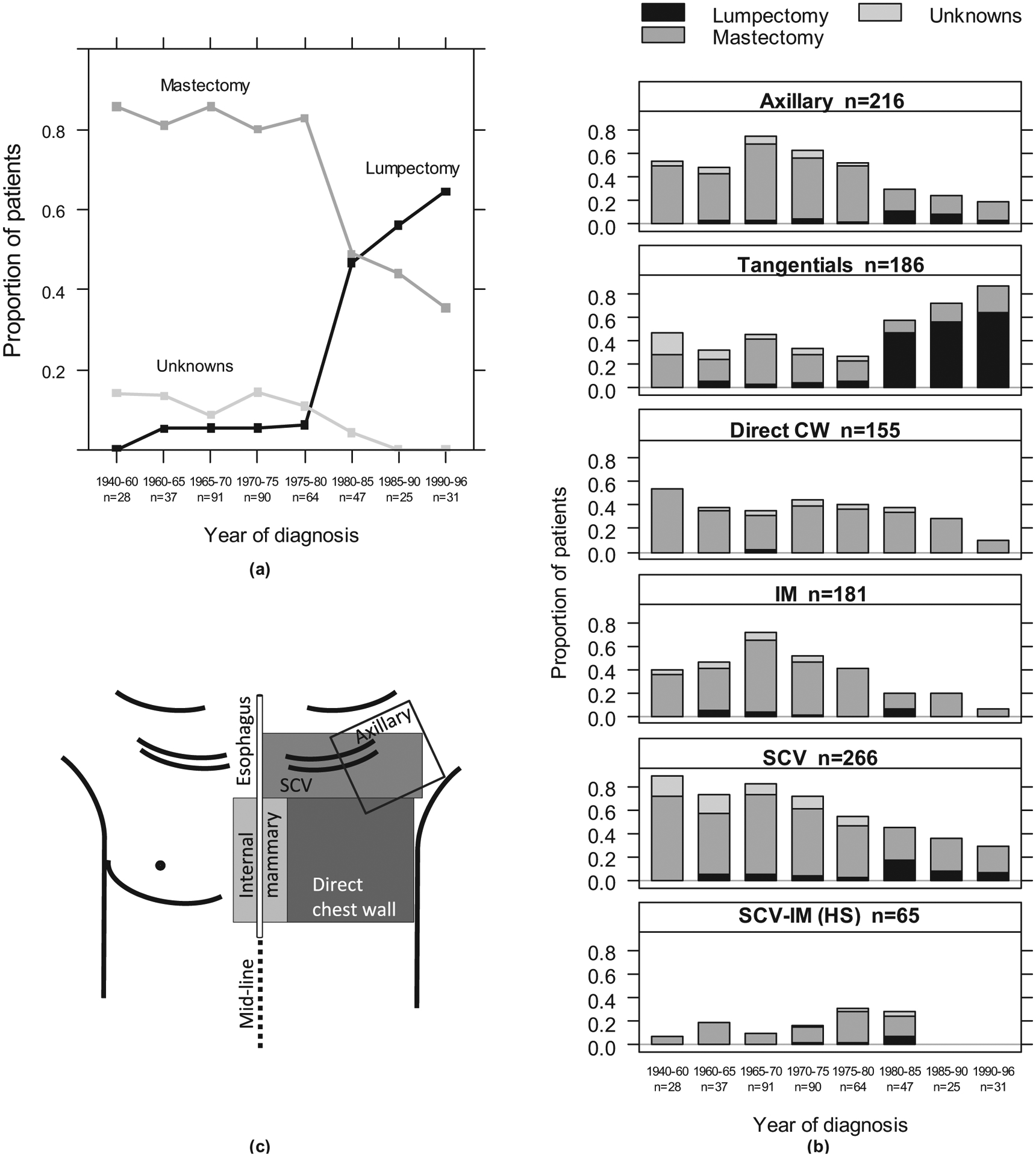
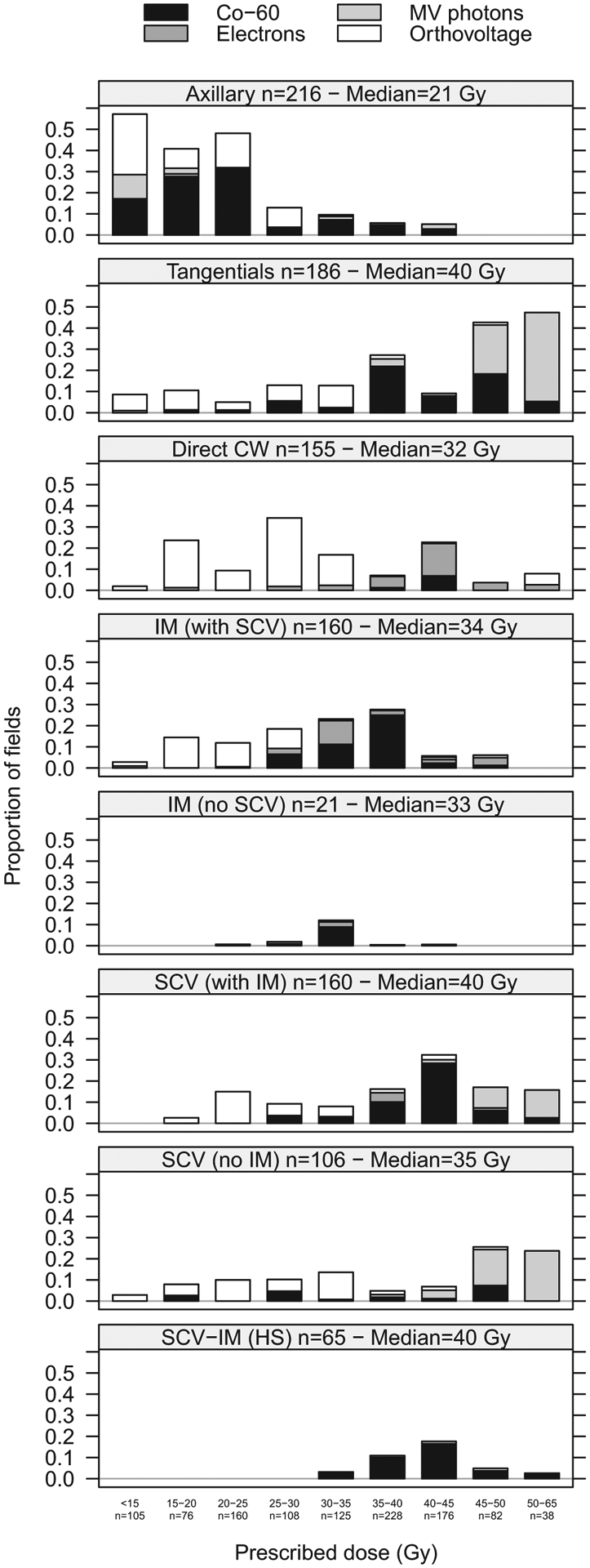
We abstracted the radiation therapy treatment parameters from each patient's radiation therapy record. Treatment fields included direct chest wall (37% of patients), medial and lateral tangentials (45%), supraclavicular (SCV, 64%), internal mammary (IM, 44%), SCV and IM together (16%), axillary (52%), and breast/chest wall boosts (7%). The beam types used were (60)Co (45% of fields), orthovoltage (33%), megavoltage photons (11%), and electrons (10%). The population median prescribed dose to the target volume ranged from 21 Gy to 40 Gy. We reconstructed the doses over the length of the esophagus using abstracted patient data, water phantom measurements, and a computational model of the human body.
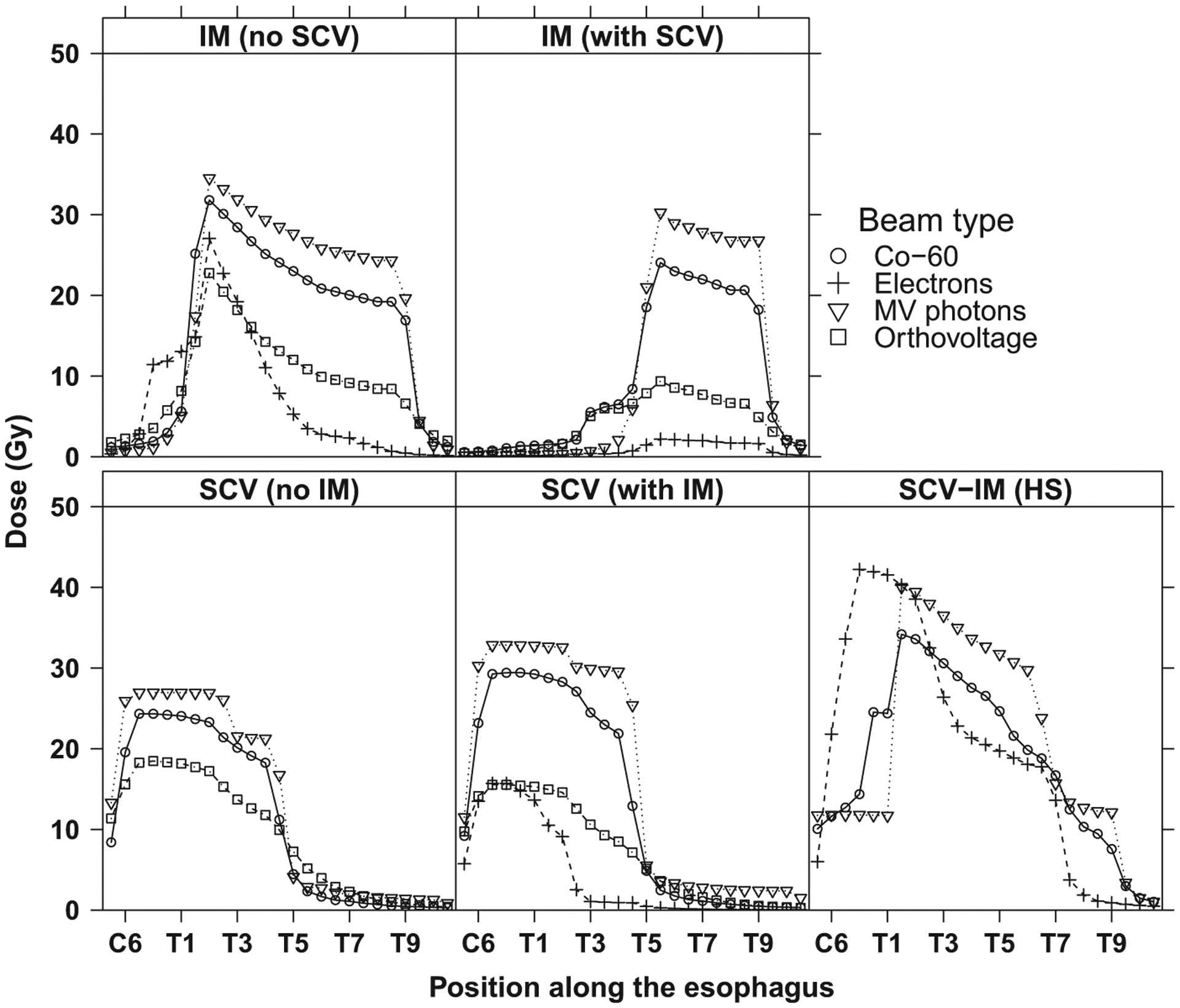
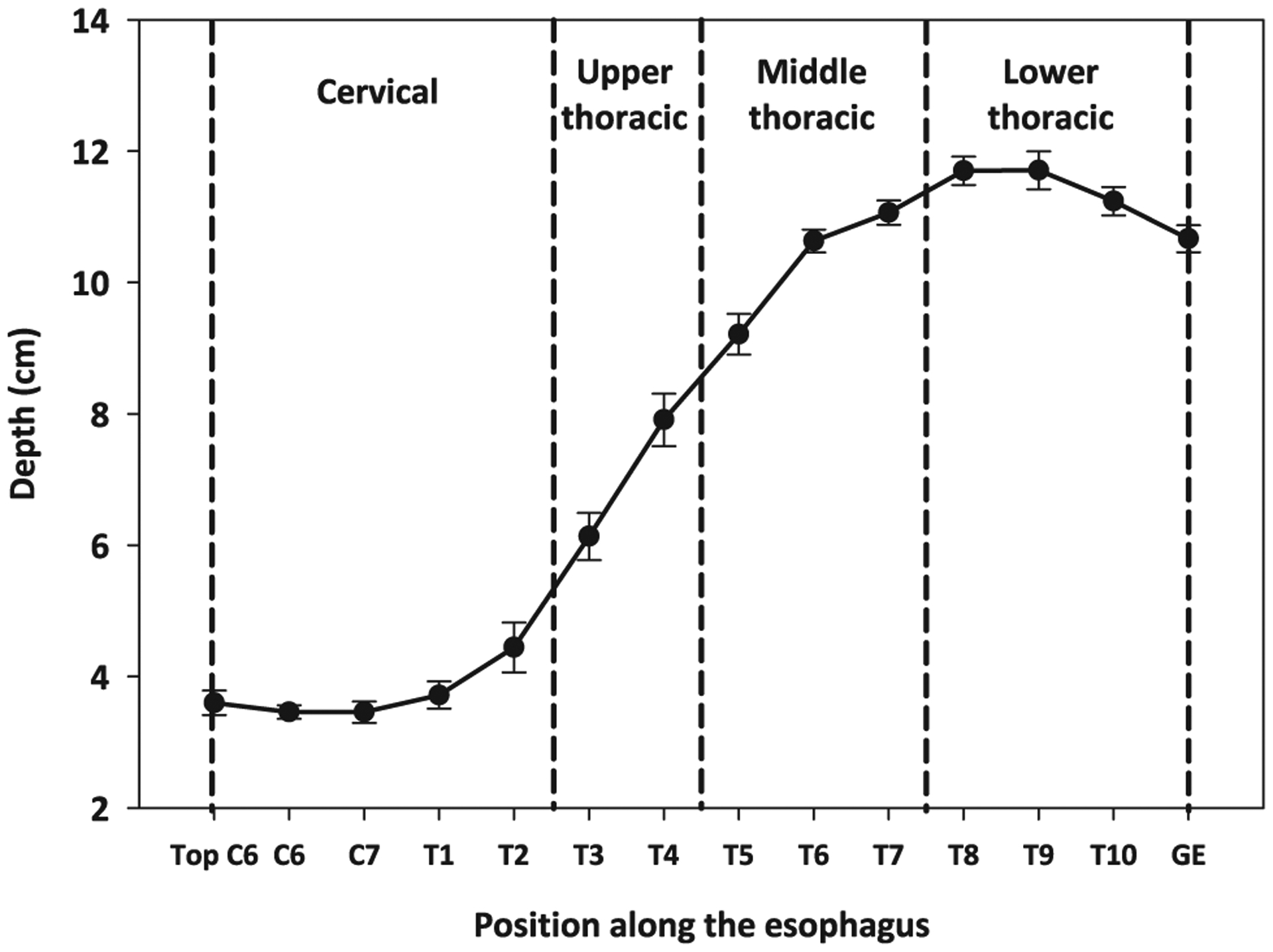
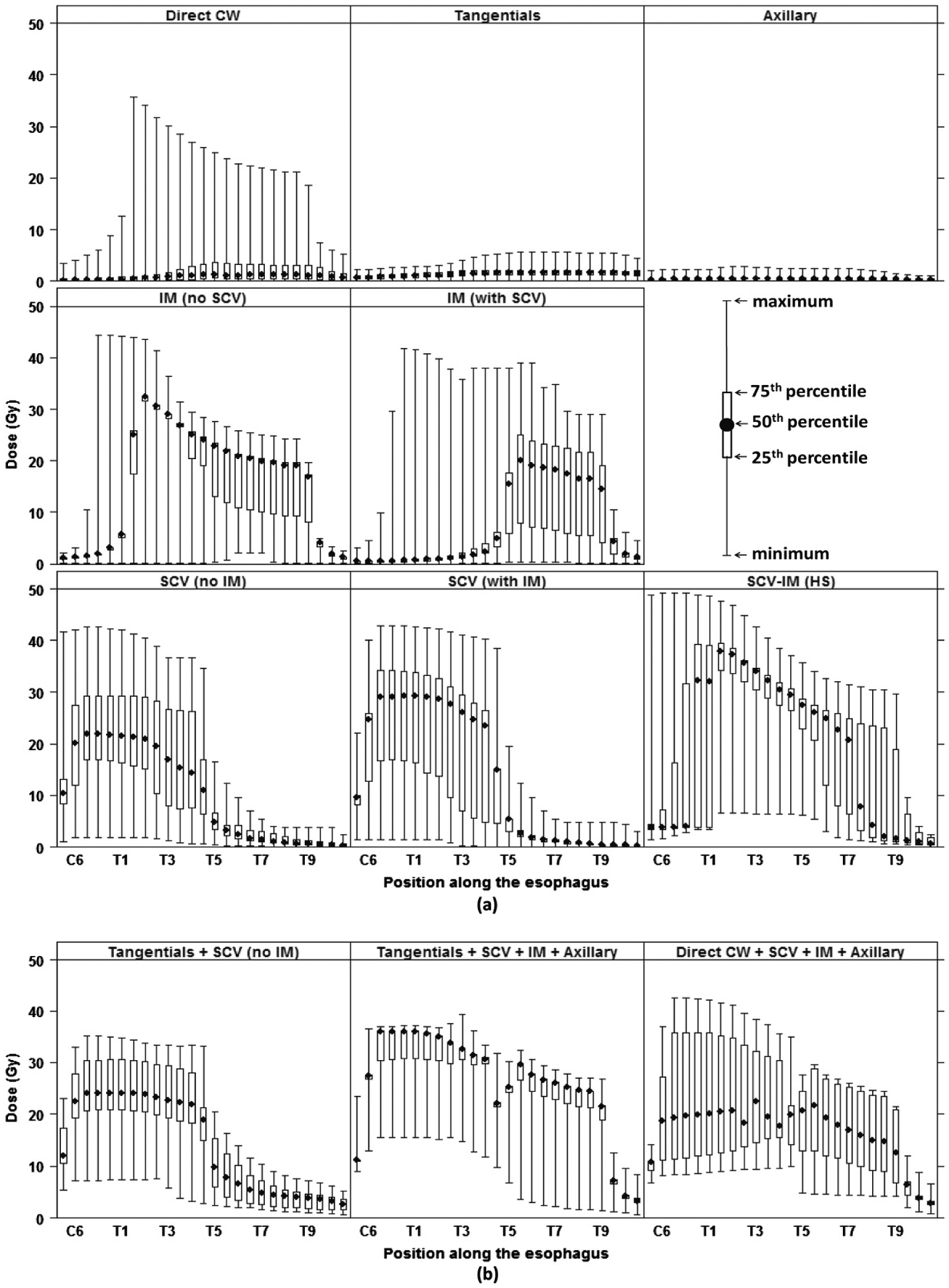
Fields that treated the SCV and/or IM lymph nodes were used for 85% of the patients and delivered the highest doses within 3 regions of the esophagus: cervical (population median 38 Gy), upper thoracic (32 Gy), and middle thoracic (25 Gy). Other fields (direct chest wall, tangential, and axillary) contributed substantially lower doses (approximately 2 Gy). The cervical to middle thoracic esophagus received the highest dose because of its close proximity to the SCV and IM fields and less overlying tissue in that part of the chest. The location of the SCV field border relative to the midline was one of the most important determinants of the dose to the esophagus.
Breast cancer patients in this study received relatively high incidental radiation therapy doses to the esophagus when the SCV and/or IM lymph nodes were treated, whereas direct chest wall, tangentials, and axillary fields contributed lower doses.
为了对北美和欧洲的 414 名因乳腺癌接受放射治疗的女性进行一项关于乳腺癌幸存者发生第二原发食管癌风险的流行病学研究,我们提供了食管的意外照射剂量学数据。
我们从每位患者的放射治疗记录中提取放射治疗参数。治疗野包括直接胸壁(37%的患者)、内侧和外侧切线野(45%)、锁骨上野(SCV,64%)、内乳野(IM,44%)、SCV 和 IM 联合野(16%)、腋窝野(52%)和乳腺/胸壁加量野(7%)。使用的射线类型包括(60)Co(45%的野)、常规放疗(33%)、兆伏光子(11%)和电子线(10%)。靶区规定的人群中位剂量范围从 21 Gy 到 40 Gy。我们使用提取的患者数据、水模测量和人体计算模型来重建食管长度上的剂量。
85%的患者使用治疗 SCV 和/或 IM 淋巴结的野来治疗,这些野在食管的 3 个区域内给予最高剂量:颈段(人群中位值 38 Gy)、胸上段(32 Gy)和胸中段(25 Gy)。其他野(直接胸壁、切线野和腋窝野)给予的剂量要低得多(约 2 Gy)。颈段到胸中段食管接受的剂量最高,因为它靠近 SCV 和 IM 野,而且胸部该部位的覆盖组织较少。SCV 野边界相对于中线的位置是决定食管剂量的最重要因素之一。
当治疗 SCV 和/或 IM 淋巴结时,本研究中的乳腺癌患者接受了相对较高的食管意外放射治疗剂量,而直接胸壁、切线野和腋窝野给予的剂量较低。