Tsai Chiaojung Jillian, Li Jing, Gonzalez-Angulo Ana M, Allen Pamela K, Woodward Wendy A, Ueno Naoto T, Lucci Anthony, Krishnamurthy Savitri, Gong Yun, Yang Wei, Cristofanilli Massimo, Valero Vicente, Buchholz Thomas A
Departments of *Radiation Oncology †Breast Medical Oncology §Surgical Oncology ∥Pathology ¶Diagnostic Radiology ‡Morgan Welch Inflammatory Breast Cancer Research Program and Clinic, The University of Texas MD Anderson Cancer Center, Houston, TX.
Am J Clin Oncol. 2015 Jun;38(3):242-7. doi: 10.1097/COC.0b013e3182937921.
We previously reported survival trends among patients with inflammatory breast cancer (IBC) over a 30-year period before 2005. Here we evaluated survival outcomes for women with IBC diagnosed before or after October 2006, in the era of HER2-directed therapy and after opening a dedicated multidisciplinary IBC clinic.
We retrospectively identified and reviewed 260 patients with newly diagnosed IBC without distant metastasis, 168 treated before October 2006 and 92 treated afterward. Most patients received anthracycline and taxane-based neoadjuvant chemotherapy, mastectomy, and postmastectomy radiation. Survival outcomes were compared between the 2 groups.
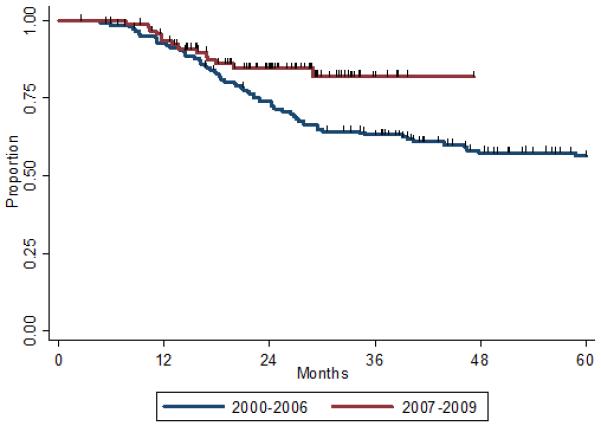
Median follow-up time was 29 months for the entire cohort (39 and 24 mo for patients treated before and after October 2006). Patients treated more recently were more likely to have received neoadjuvant HER2-directed therapy for HER2-positive tumors (100% vs. 54%, P=0.001). No differences were found in receipt of hormone therapy. Three-year overall survival rates were 63% for those treated before and 82% for those treated after October 2006 (log-rank P=0.02). Univariate Cox analysis demonstrated better overall survival among patients treated after October 2006 than among those treated beforehand (hazard ratio [HR] 0.5; 95% confidence interval [CI], 0.34-0.94); a trend toward improved survival was noted in the multivariate analysis (HR=0.47; 95% CI, 0.19-1.16; P=0.10). Significant factors in the multivariate model included HER2-directed therapy (HR=0.38; 95% CI, 0.17-0.84; P=0.02) and estrogen receptor positivity (HR=0.32; 95% CI, 0.14-0.74; P=0.01).
Survival improved in the context of the IBC clinic and prompt initiation of neoadjuvant HER2-directed therapeutics.
我们之前报告了2005年之前30年间炎性乳腺癌(IBC)患者的生存趋势。在此,我们评估了2006年10月之前或之后确诊的IBC女性患者在HER2靶向治疗时代以及开设专门的多学科IBC诊所后的生存结果。
我们回顾性地识别并审查了260例新诊断为无远处转移的IBC患者,其中168例在2006年10月之前接受治疗,92例在之后接受治疗。大多数患者接受了基于蒽环类和紫杉烷的新辅助化疗、乳房切除术以及乳房切除术后放疗。比较两组的生存结果。
整个队列的中位随访时间为29个月(2006年10月之前和之后接受治疗的患者分别为39个月和24个月)。近期接受治疗的患者更有可能接受针对HER2阳性肿瘤的新辅助HER2靶向治疗(100%对54%,P = 0.001)。在接受激素治疗方面未发现差异。2006年10月之前接受治疗的患者3年总生存率为63%,2006年10月之后接受治疗的患者为82%(对数秩检验P = 0.02)。单因素Cox分析显示,2006年10月之后接受治疗的患者总体生存率优于之前接受治疗的患者(风险比[HR] 0.5;95%置信区间[CI],0.34 - 0.94);多因素分析中观察到生存改善的趋势(HR = 0.47;95% CI,0.19 - 1.16;P = 0.10)。多因素模型中的显著因素包括HER2靶向治疗(HR = 0.38;95% CI,0.17 - 0.84;P = 0.02)和雌激素受体阳性(HR = 0.32;95% CI,0.14 - 0.74;P = 0.01)。
在IBC诊所的背景下以及新辅助HER2靶向治疗的迅速启动,生存情况有所改善。