University of Utah School of Medicine, 30 N 1900 E, Salt Lake City, UT 84132, USA.
JAMA. 2013 May 15;309(19):2016-24. doi: 10.1001/jama.2013.4919.
More than 225 000 surgeries are performed annually in the United States for pelvic organ prolapse (POP). Abdominal sacrocolpopexy is considered the most durable POP surgery, but little is known about safety and long-term effectiveness.
To describe anatomic and symptomatic outcomes up to 7 years after abdominal sacrocolpopexy, and to determine whether these are affected by concomitant anti-incontinence surgery (Burch urethropexy).
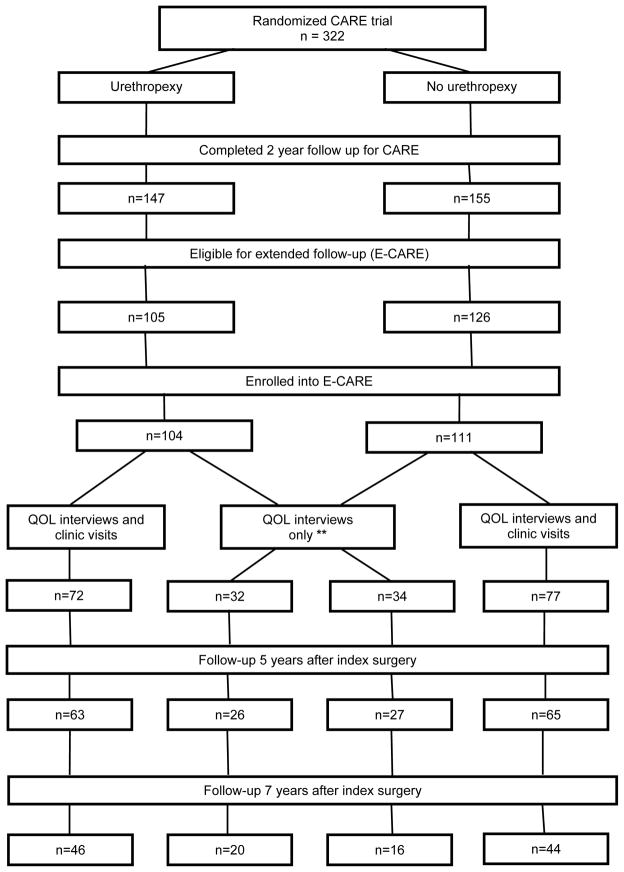
DESIGN, SETTING, AND PARTICIPANTS: Long-term follow-up of the randomized, masked 2-year Colpopexy and Urinary Reduction Efforts (CARE) trial of women with stress continence who underwent abdominal sacrocolpopexy between 2002 and 2005 for symptomatic POP and also received either concomitant Burch urethropexy or no urethropexy. Ninety-two percent (215/233) of eligible 2-year CARE trial completers were enrolled in the extended CARE study; and 181 (84%) and 126 (59%) completed 5 and 7 years of follow-up, respectively. The median follow-up was 7 years.
Symptomatic POP failure requiring retreatment or self-reported bulge; or anatomic POP failure requiring retreatment or Pelvic Organ Prolapse Quantification evaluation demonstrating descent of the vaginal apex below the upper third of the vagina, or anterior or posterior vaginal wall prolapse beyond the hymen. Stress urinary incontinence (SUI) with more than 1 symptom or interval treatment; or overall UI score of 3 or greater on the Incontinence Severity Index.
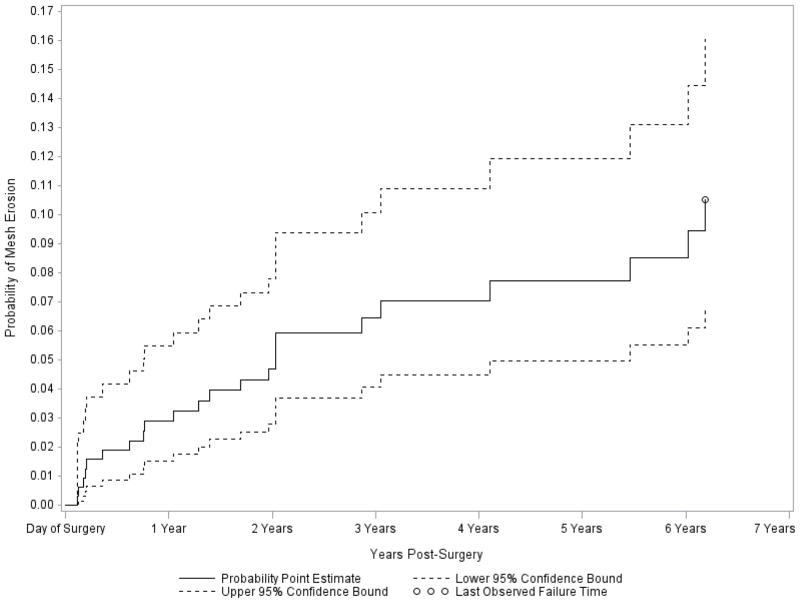
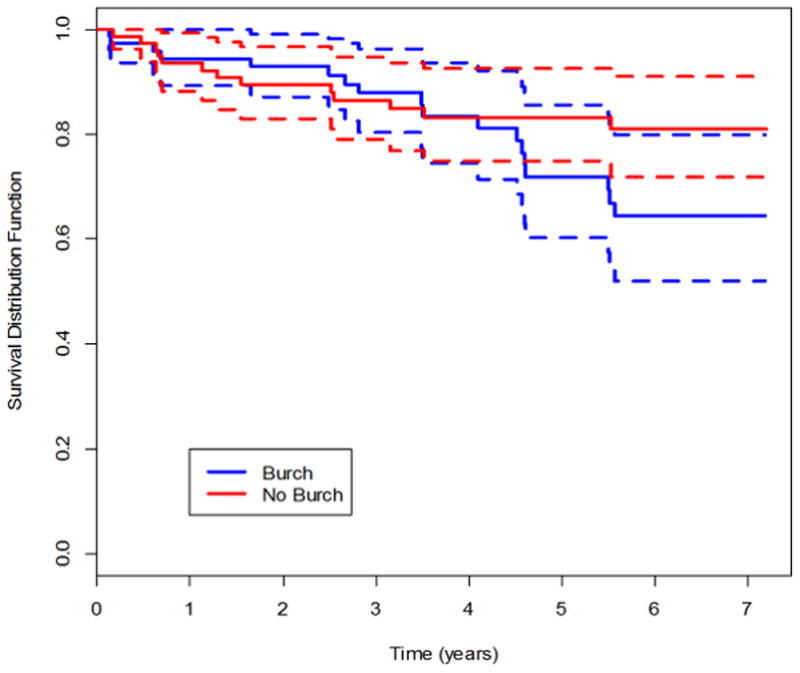
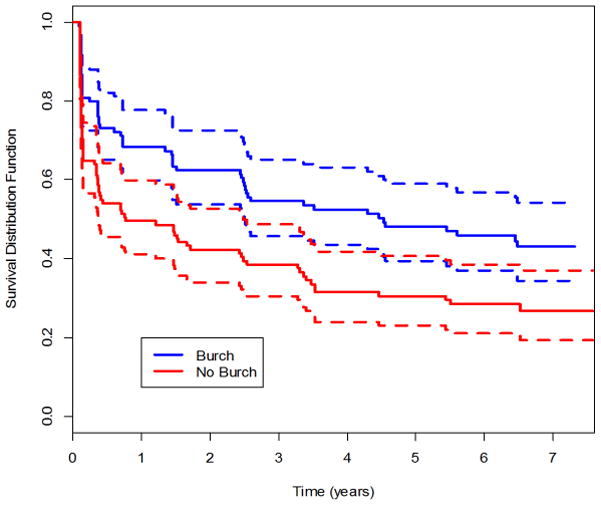
By year 7, the estimated probabilities of treatment failure (POP, SUI, UI) from parametric survival modeling for the urethropexy group and the no urethropexy group, respectively, were 0.27 and 0.22 for anatomic POP (treatment difference of 0.050; 95% CI, -0.161 to 0.271), 0.29 and 0.24 for symptomatic POP (treatment difference of 0.049; 95% CI, -0.060 to 0.162), 0.48 and 0.34 for composite POP (treatment difference of 0.134; 95% CI, -0.096 to 0.322), 0.62 and 0.77 for SUI (treatment difference of -0.153; 95% CI, -0.268 to 0.030), and 0.75 and 0.81 for overall UI (treatment difference of -0.064; 95% CI, -0.161 to 0.032). Mesh erosion probability at 7 years (estimated by the Kaplan-Meier method) was 10.5% (95% CI, 6.8% to 16.1%).
During 7 years of follow-up, abdominal sacrocolpopexy failure rates increased in both groups. Urethropexy prevented SUI longer than no urethropexy. Abdominal sacrocolpopexy effectiveness should be balanced with long-term risks of mesh or suture erosion.
clinicaltrials.gov Identifier: NCT00099372.
在美国,每年有超过 225000 例手术用于治疗盆腔器官脱垂(POP)。腹式骶骨阴道固定术被认为是最持久的 POP 手术,但对于其安全性和长期效果知之甚少。
描述腹式骶骨阴道固定术后 7 年的解剖和症状结果,并确定这些结果是否受到同时进行的抗失禁手术(Burch 尿道悬吊术)的影响。
设计、地点和参与者:对 2002 年至 2005 年间接受腹式骶骨阴道固定术治疗有压力性尿失禁的女性进行的随机、双盲、为期 2 年的 Colpopexy 和尿失禁减少效果(CARE)试验的长期随访。这些女性患有症状性 POP,并同时接受了 Burch 尿道悬吊术或不接受尿道悬吊术。符合条件的 2 年 CARE 试验完成者中,92%(215/233)被纳入扩展 CARE 研究;181 人(84%)和 126 人(59%)分别完成了 5 年和 7 年的随访。中位随访时间为 7 年。
需要再次治疗或自我报告膨出的症状性 POP 失败;或需要再次治疗或盆腔器官脱垂定量评估显示阴道顶点下降至阴道上三分之一以下,或阴道前壁或后壁脱垂至处女膜以外的解剖性 POP 失败。有超过 1 个症状或间隔治疗的压力性尿失禁(SUI);或失禁严重程度指数(Incontinence Severity Index)得分为 3 或更高的整体尿失禁。
通过参数生存模型估计,在尿道悬吊组和无尿道悬吊组中,7 年时的治疗失败(POP、SUI、UI)的估计概率分别为解剖性 POP 0.27 和 0.22(治疗差异 0.050;95%CI,-0.161 至 0.271)、症状性 POP 0.29 和 0.24(治疗差异 0.049;95%CI,-0.060 至 0.162)、复合 POP 0.48 和 0.34(治疗差异 0.134;95%CI,-0.096 至 0.322)、SUI 0.62 和 0.77(治疗差异-0.153;95%CI,-0.268 至 0.030)和整体 UI 0.75 和 0.81(治疗差异-0.064;95%CI,-0.161 至 0.032)。7 年时(通过 Kaplan-Meier 方法估计)的网片侵蚀概率为 10.5%(95%CI,6.8%至 16.1%)。
在 7 年的随访期间,两组的腹式骶骨阴道固定术失败率都有所增加。尿道悬吊术比无尿道悬吊术更能预防 SUI。应权衡腹式骶骨阴道固定术的有效性与长期网片或缝线侵蚀的风险。
clinicaltrials.gov 标识符:NCT00099372。