Department of Radiation Oncology, National Cancer Center Hospital, Tokyo, Japan.
J Radiat Res. 2013 Nov 1;54(6):1146-52. doi: 10.1093/jrr/rrt072. Epub 2013 May 31.
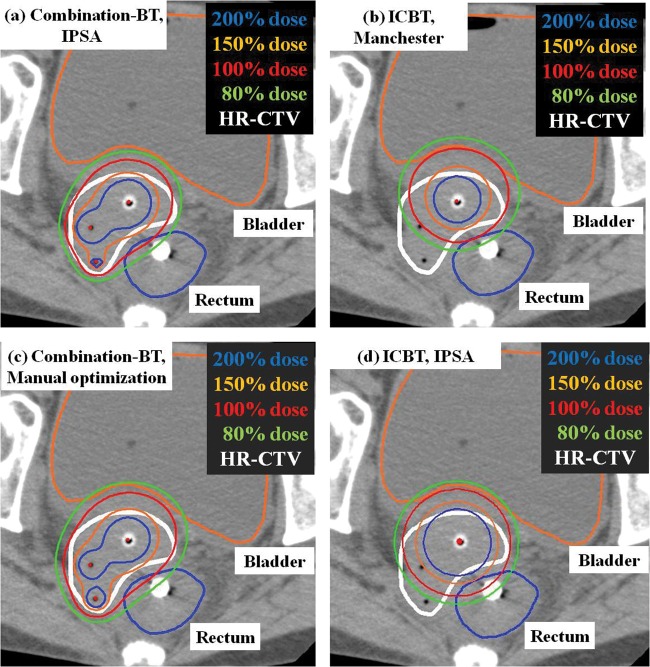
The main purpose of this study was to compare three different treatment plans for locally advanced cervical cancer: (i) the inverse-planning simulated annealing (IPSA) plan for combination brachytherapy (BT) of interstitial and intracavitary brachytherapy, (ii) manual optimization based on the Manchester system for combination-BT, and (iii) the conventional Manchester system using only tandem and ovoids. This was a retrospective study of 25 consecutive implants. The high-risk clinical target volume (HR-CTV) and organs at risk were defined according to the GEC-ESTRO Working Group definitions. A dose of 6 Gy was prescribed. The uniform cost function for dose constraints was applied to all IPSA-generated plans. The coverage of the HR-CTV by IPSA for combination-BT was equivalent to that of manual optimization, and was better than that of the Manchester system using only tandem and ovoids. The mean V100 achieved by IPSA for combination-BT, manual optimization and Manchester was 96 ± 3.7%, 95 ± 5.5% and 80 ± 13.4%, respectively. The mean D100 was 483 ± 80, 487 ± 97 and 335 ± 119 cGy, respectively. The mean D90 was 677 ± 61, 681 ± 88 and 513 ± 150 cGy, respectively. IPSA resulted in significant reductions of the doses to the rectum (IPSA D2cm(3): 408 ± 71 cGy vs manual optimization D2cm(3): 485 ± 105 cGy; P = 0.03) and the bladder (IPSA D2cm(3): 452 ± 60 cGy vs manual optimization D2cm(3): 583 ± 113 cGy; P < 0.0001). In conclusion, combination-BT achieved better tumor coverage, and plans using IPSA provided significant sparing of normal tissues without compromising CTV coverage.
(i)间质和腔内近距离治疗联合的逆规划模拟退火(IPSA)计划,(ii)基于曼彻斯特系统的联合-BT 手动优化,以及(iii)仅使用尾翼和卵圆的传统曼彻斯特系统。这是一项回顾性研究,共纳入 25 例连续植入患者。高危临床靶区(HR-CTV)和危及器官根据 GEC-ESTRO 工作组的定义进行定义。规定 6 Gy 剂量。所有 IPSA 生成的计划均应用均匀成本函数来满足剂量限制。IPSA 用于联合-BT 的 HR-CTV 覆盖范围与手动优化相当,优于仅使用尾翼和卵圆的曼彻斯特系统。IPSA 用于联合-BT、手动优化和曼彻斯特系统的 HR-CTV 的平均 V100 分别为 96±3.7%、95±5.5%和 80±13.4%。平均 D100 分别为 483±80、487±97 和 335±119 cGy。平均 D90 分别为 677±61、681±88 和 513±150 cGy。IPSA 可显著降低直肠(IPSA D2cm(3):408±71 cGy 比手动优化 D2cm(3):485±105 cGy;P=0.03)和膀胱(IPSA D2cm(3):452±60 cGy 比手动优化 D2cm(3):583±113 cGy;P<0.0001)的剂量。总之,联合-BT 可实现更好的肿瘤覆盖,而 IPSA 计划则可在不影响 CTV 覆盖的情况下显著保护正常组织。