Department of Epidemiology, Harvard School of Public Health, Boston, Massachusetts, USA.
PLoS One. 2013 May 29;8(5):e64636. doi: 10.1371/journal.pone.0064636. Print 2013.
Child undernutrition affects millions of children globally. We investigated associations between suboptimal growth and mortality by pooling large studies.
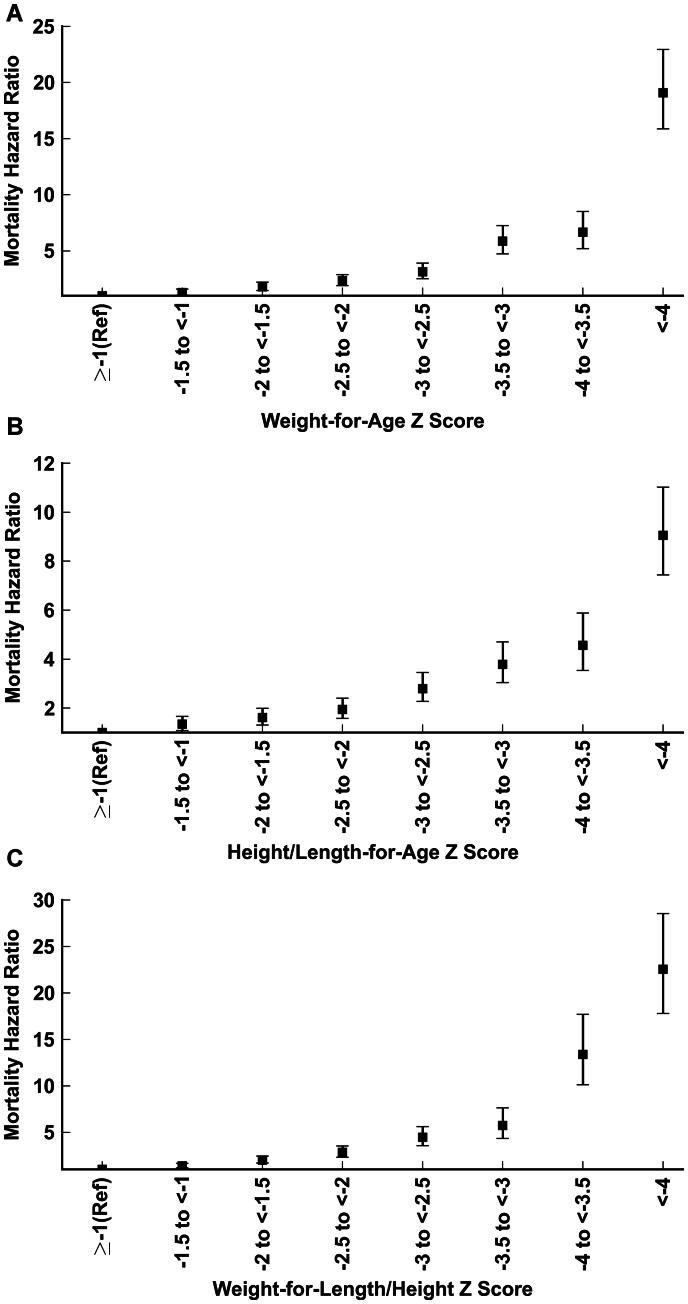
Pooled analysis involving children 1 week to 59 months old in 10 prospective studies in Africa, Asia and South America. Utilizing most recent measurements, we calculated weight-for-age, height/length-for-age and weight-for-height/length Z scores, applying 2006 WHO Standards and the 1977 NCHS/WHO Reference. We estimated all-cause and cause-specific mortality hazard ratios (HR) using proportional hazards models comparing children with mild (-2≤Z<-1), moderate (-3≤Z<-2), or severe (Z<-3) anthropometric deficits with the reference category (Z≥-1).
53 809 children were eligible for this re-analysis and contributed a total of 55 359 person-years, during which 1315 deaths were observed. All degrees of underweight, stunting and wasting were associated with significantly higher mortality. The strength of association increased monotonically as Z scores decreased. Pooled mortality HR was 1.52 (95% Confidence Interval 1.28, 1.81) for mild underweight; 2.63 (2.20, 3.14) for moderate underweight; and 9.40 (8.02, 11.03) for severe underweight. Wasting was a stronger determinant of mortality than stunting or underweight. Mortality HR for severe wasting was 11.63 (9.84, 13.76) compared with 5.48 (4.62, 6.50) for severe stunting. Using older NCHS standards resulted in larger HRs compared with WHO standards. In cause-specific analyses, all degrees of anthropometric deficits increased the hazards of dying from respiratory tract infections and diarrheal diseases. The study had insufficient power to precisely estimate effects of undernutrition on malaria mortality.
All degrees of anthropometric deficits are associated with increased risk of under-five mortality using the 2006 WHO Standards. Even mild deficits substantially increase mortality, especially from infectious diseases.
儿童营养不足影响着全球数以百万计的儿童。我们通过汇集大型研究来调查生长发育不良与死亡率之间的关联。
纳入非洲、亚洲和南美洲 10 项前瞻性研究中 1 周至 59 月龄的儿童进行汇总分析。利用最近的测量值,我们计算体重/年龄、身高/长度/年龄和体重/身高/长度 Z 分数,采用 2006 年世卫组织标准和 1977 年 NCHS/WHO 参考标准。我们使用比例风险模型比较有轻度(-2≤Z<-1)、中度(-3≤Z<-2)或重度(Z<-3)生长发育不良的儿童与参考组(Z≥-1),估计全因和病因特异性死亡率风险比(HR)。
53809 名儿童符合重新分析标准,共纳入 55359 人年,在此期间观察到 1315 例死亡。所有程度的消瘦、发育迟缓及消瘦均与死亡率显著升高相关。随着 Z 分数的降低,关联强度呈单调递增。轻度消瘦的汇总死亡率 HR 为 1.52(95%置信区间 1.28,1.81);中度消瘦为 2.63(2.20,3.14);重度消瘦为 9.40(8.02,11.03)。消瘦比发育迟缓或消瘦是死亡率更强的决定因素。与严重发育迟缓相比,严重消瘦的死亡率 HR 为 11.63(9.84,13.76),而严重发育迟缓的死亡率 HR 为 5.48(4.62,6.50)。与世卫组织标准相比,使用旧的 NCHS 标准会产生更大的 HR。在病因特异性分析中,所有程度的生长发育不良均增加了死于呼吸道感染和腹泻病的风险。本研究的效力不足以准确估计营养不良对疟疾死亡率的影响。
使用 2006 年世卫组织标准,所有程度的生长发育不良都与五岁以下儿童死亡率升高相关。即使是轻度的发育不良也会显著增加死亡率,尤其是因传染病导致的死亡率。