Centre of Research Excellence to Reduce Inequality in Heart Disease, Preventative Health, Baker IDI Heart and Diabetes Institute, Melbourne, Australia.
PLoS One. 2013 May 29;8(5):e65795. doi: 10.1371/journal.pone.0065795. Print 2013.
Gender-based clinical differences are increasingly being identified as having significant influence on the outcomes of patients with cardiovascular disease (CVD), including atrial fibrillation (AF).
To perform detailed clinical phenotyping on a cohort of hospitalised patients with chronic forms of AF to understand if gender-based differences exist in the clinical presentation, thrombo-embolic risk and therapeutic management of high risk patients hospitalised with chronic AF.
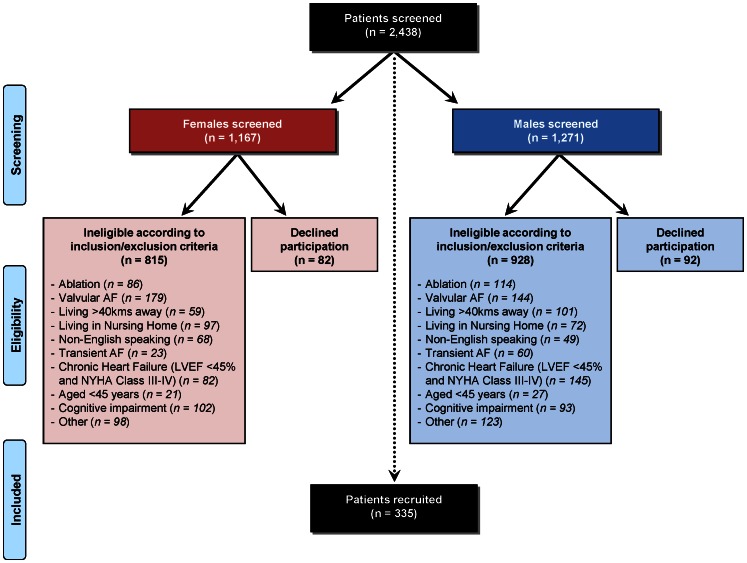
We are undertaking the Standard versus Atrial Fibrillation spEcific managemenT studY (SAFETY) - a multi-centre, randomised controlled trial of an AF-specific management intervention versus usual care. Extensive baseline profiling of recruited patients was undertaken to identify gender-specific differences for risk delineation.
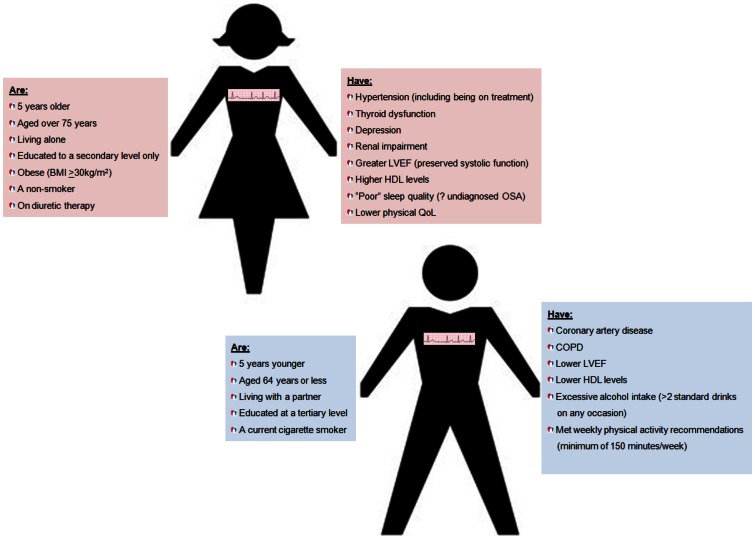
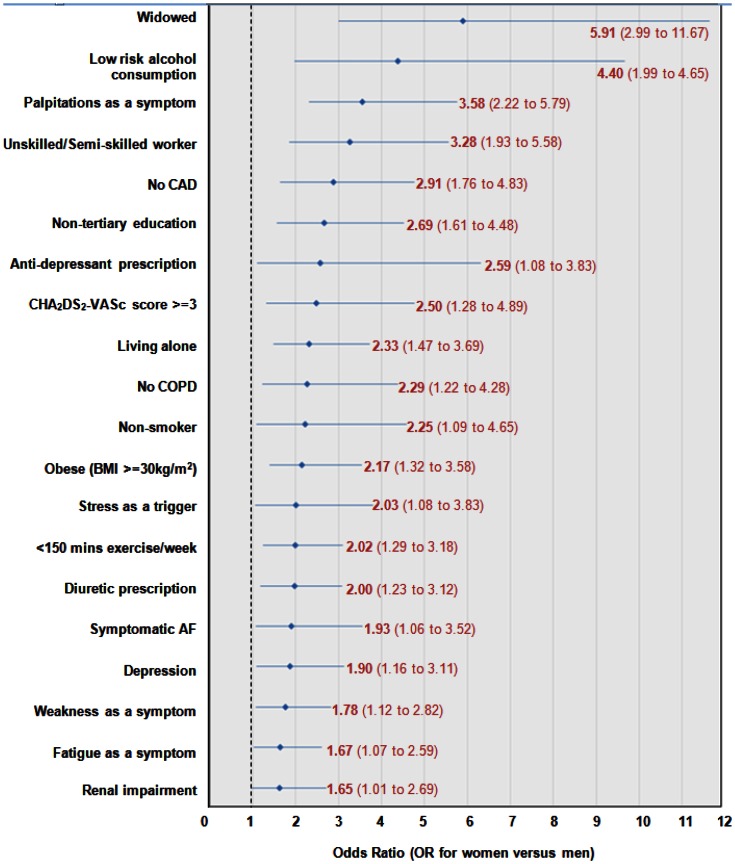
We screened 2,438 patients with AF and recruited 335 into SAFETY. Of these, 48.1% were women who were, on average, 5 years older than their male counterparts. Women and men displayed divergent antecedent profiles, with women having a higher thrombo-embolic risk but being prescribed similar treatment regimens. More women than men presented to hospital with co-morbid thyroid dysfunction, depression, renal impairment and obesity. In contrast, more men presented with coronary artery disease (CAD) and/or chronic obstructive pulmonary disease (COPD). Even when data was age-adjusted, women were more likely to live alone (odds ratio [OR] 2.33; 95% confidence interval [CI] 1.47 to 3.69), have non-tertiary education (OR 2.69; 95% CI 1.61 to 4.48) and be symptomatic (OR 1.93; 95% CI 1.06 to 3.52).
Health care providers should be cognisant of gender-specific differences in an attempt to individualise and, hence, optimise the management of patients with chronic AF and reduce potential morbidity and mortality.
性别相关的临床差异正日益被认为对心血管疾病(CVD)患者的治疗效果有重大影响,包括房颤(AF)患者。
对一组慢性 AF 住院患者进行详细的临床表型分析,以了解性别差异是否存在于高危慢性 AF 住院患者的临床表现、血栓栓塞风险和治疗管理中。
我们正在进行标准与房颤特异性管理研究(SAFETY)-一项房颤特异性管理干预与常规护理的多中心随机对照试验。对招募的患者进行广泛的基线特征分析,以确定性别特异性风险特征。
我们筛查了 2438 例 AF 患者,其中 335 例入选 SAFETY。其中,48.1%为女性,平均比男性年长 5 岁。女性和男性表现出不同的既往病史特征,女性的血栓栓塞风险更高,但接受的治疗方案相似。与男性相比,更多的女性因合并甲状腺功能障碍、抑郁、肾功能不全和肥胖而住院。相比之下,更多的男性因冠心病(CAD)和/或慢性阻塞性肺疾病(COPD)而住院。即使对数据进行年龄调整,女性更有可能独居(比值比[OR]2.33;95%置信区间[CI]1.47-3.69)、接受非高等教育(OR 2.69;95%CI 1.61-4.48)和有症状(OR 1.93;95%CI 1.06-3.52)。
医疗保健提供者应认识到性别差异,试图实现个体化治疗,从而优化慢性 AF 患者的管理,降低潜在的发病率和死亡率。