Institute for Health Metrics and Evaluation, Seattle, WA 98121, USA.
Lancet. 2012 Dec 15;380(9859):2224-60. doi: 10.1016/S0140-6736(12)61766-8.
Quantification of the disease burden caused by different risks informs prevention by providing an account of health loss different to that provided by a disease-by-disease analysis. No complete revision of global disease burden caused by risk factors has been done since a comparative risk assessment in 2000, and no previous analysis has assessed changes in burden attributable to risk factors over time.
We estimated deaths and disability-adjusted life years (DALYs; sum of years lived with disability [YLD] and years of life lost [YLL]) attributable to the independent effects of 67 risk factors and clusters of risk factors for 21 regions in 1990 and 2010. We estimated exposure distributions for each year, region, sex, and age group, and relative risks per unit of exposure by systematically reviewing and synthesising published and unpublished data. We used these estimates, together with estimates of cause-specific deaths and DALYs from the Global Burden of Disease Study 2010, to calculate the burden attributable to each risk factor exposure compared with the theoretical-minimum-risk exposure. We incorporated uncertainty in disease burden, relative risks, and exposures into our estimates of attributable burden.
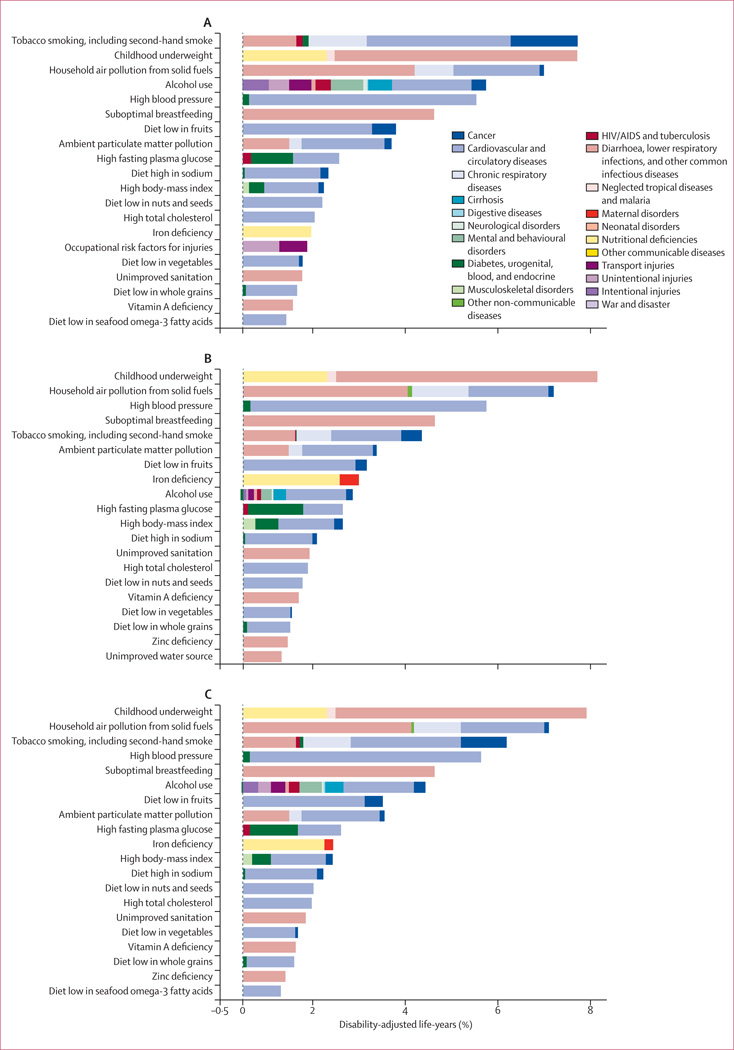
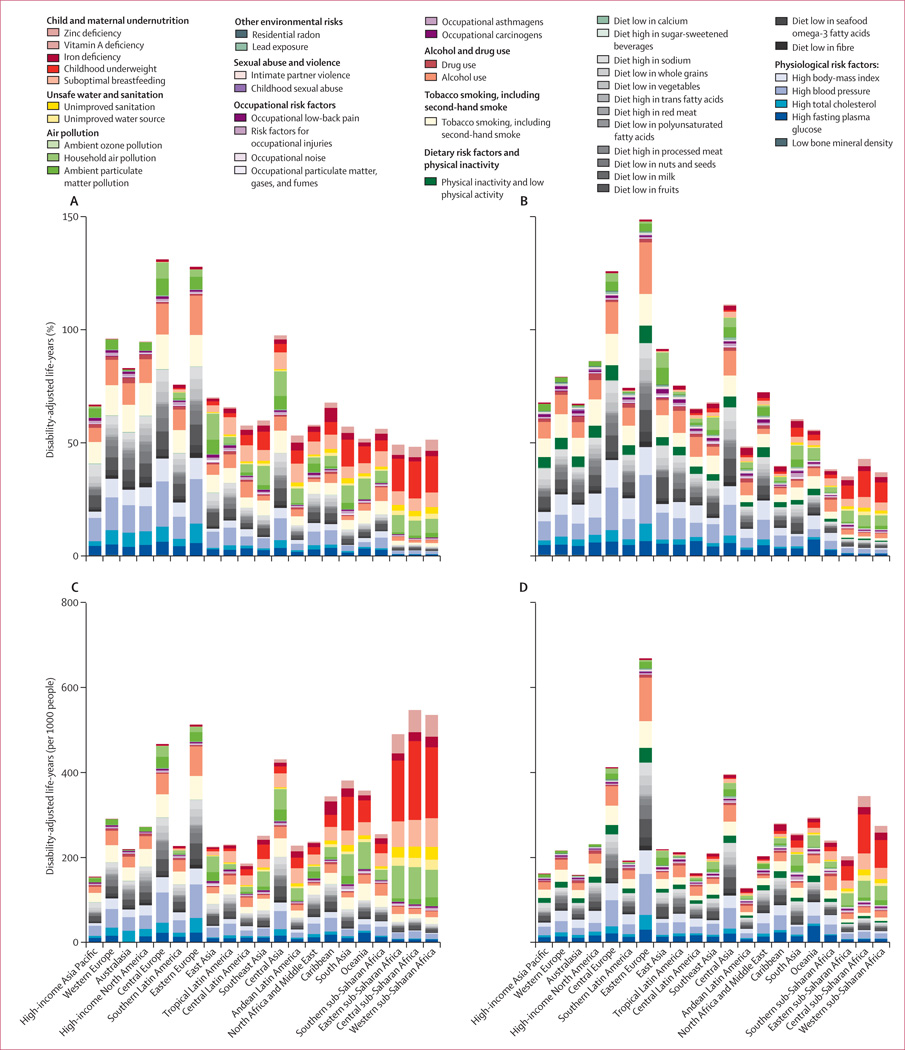
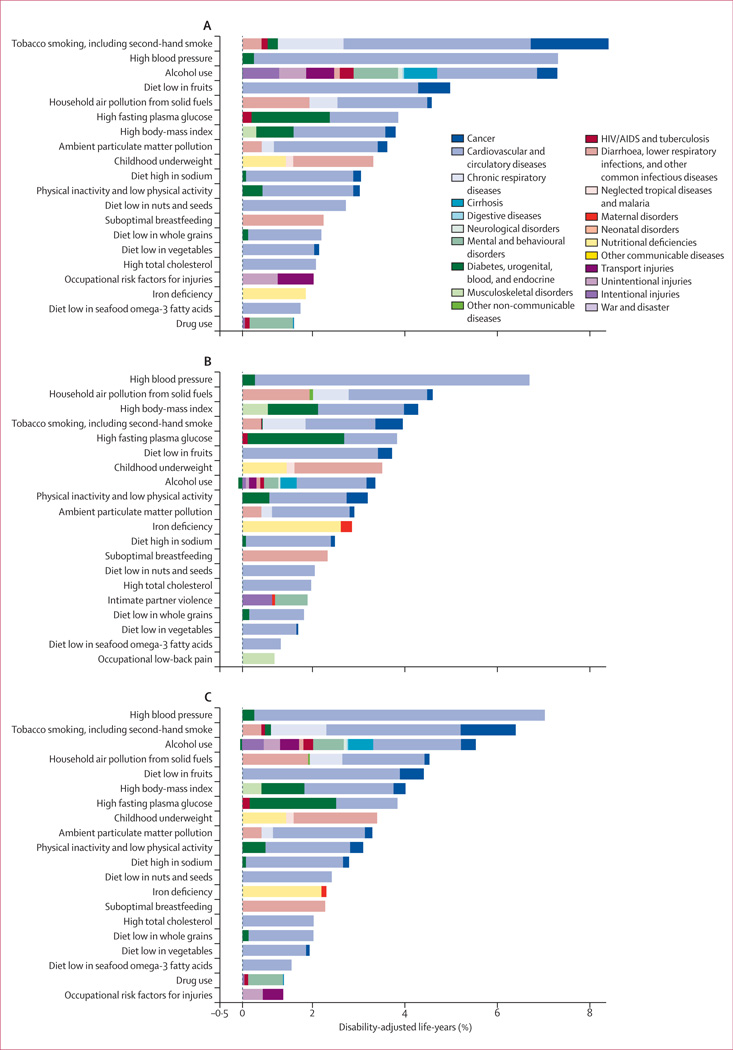
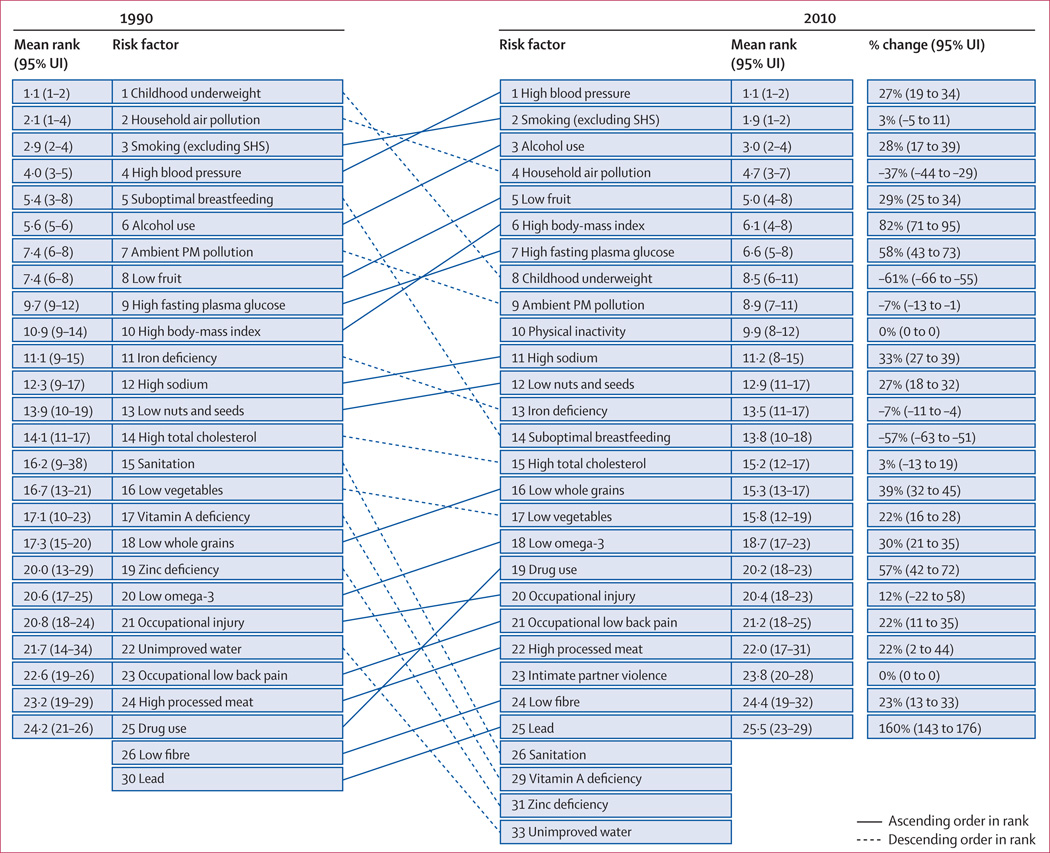
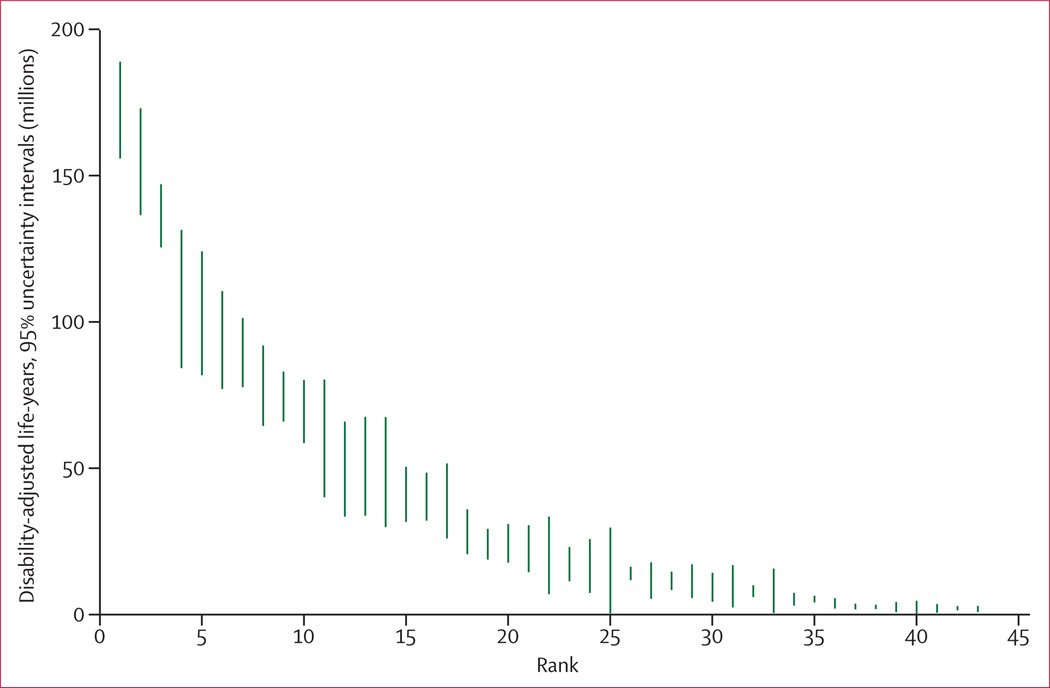
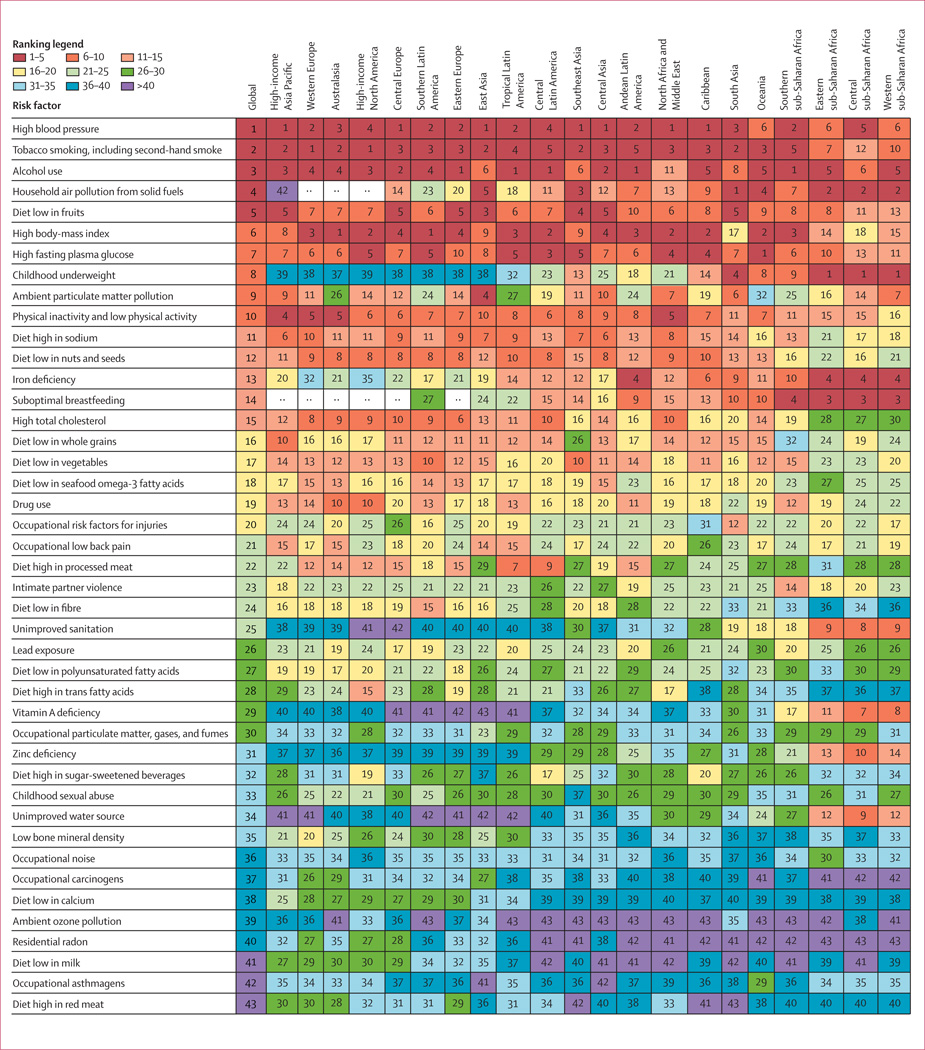
In 2010, the three leading risk factors for global disease burden were high blood pressure (7·0% [95% uncertainty interval 6·2-7·7] of global DALYs), tobacco smoking including second-hand smoke (6·3% [5·5-7·0]), and alcohol use (5·5% [5·0-5·9]). In 1990, the leading risks were childhood underweight (7·9% [6·8-9·4]), household air pollution from solid fuels (HAP; 7·0% [5·6-8·3]), and tobacco smoking including second-hand smoke (6·1% [5·4-6·8]). Dietary risk factors and physical inactivity collectively accounted for 10·0% (95% UI 9·2-10·8) of global DALYs in 2010, with the most prominent dietary risks being diets low in fruits and those high in sodium. Several risks that primarily affect childhood communicable diseases, including unimproved water and sanitation and childhood micronutrient deficiencies, fell in rank between 1990 and 2010, with unimproved water and sanitation accounting for 0·9% (0·4-1·6) of global DALYs in 2010. However, in most of sub-Saharan Africa childhood underweight, HAP, and non-exclusive and discontinued breastfeeding were the leading risks in 2010, while HAP was the leading risk in south Asia. The leading risk factor in Eastern Europe, most of Latin America, and southern sub-Saharan Africa in 2010 was alcohol use; in most of Asia, North Africa and Middle East, and central Europe it was high blood pressure. Despite declines, tobacco smoking including second-hand smoke remained the leading risk in high-income north America and western Europe. High body-mass index has increased globally and it is the leading risk in Australasia and southern Latin America, and also ranks high in other high-income regions, North Africa and Middle East, and Oceania.
Worldwide, the contribution of different risk factors to disease burden has changed substantially, with a shift away from risks for communicable diseases in children towards those for non-communicable diseases in adults. These changes are related to the ageing population, decreased mortality among children younger than 5 years, changes in cause-of-death composition, and changes in risk factor exposures. New evidence has led to changes in the magnitude of key risks including unimproved water and sanitation, vitamin A and zinc deficiencies, and ambient particulate matter pollution. The extent to which the epidemiological shift has occurred and what the leading risks currently are varies greatly across regions. In much of sub-Saharan Africa, the leading risks are still those associated with poverty and those that affect children.
Bill & Melinda Gates Foundation.
通过量化由不同风险导致的疾病负担,可以为预防措施提供不同于疾病分析的健康损失评估,从而为预防措施提供信息。自 2000 年进行比较风险评估以来,还没有对全球范围内由风险因素导致的疾病负担进行过完整的修订,也没有对随时间推移归因于风险因素的负担变化进行过分析。
我们估计了 67 个风险因素以及 21 个地区的风险因素集群在 1990 年和 2010 年对 67 个风险因素以及 21 个地区的风险因素集群导致的死亡和伤残调整生命年(DALY;失能生命年[YLD]和死亡损失生命年[YLL]之和)。我们通过系统回顾和综合已发表和未发表的数据,估计了每年、每个地区、每个性别和每个年龄组的暴露分布以及每单位暴露的相对风险。我们使用这些估计值以及 2010 年全球疾病负担研究中的特定病因死亡和 DALY 估计值,计算了与理论最小风险暴露相比,每个风险因素暴露造成的负担。我们将疾病负担、相对风险和暴露的不确定性纳入归因于负担的估计值中。
2010 年,全球疾病负担的三个主要风险因素是高血压(7.0%[95%置信区间 6.2-7.7]的全球 DALY)、包括二手烟在内的烟草使用(6.3%[5.5-7.0%])和饮酒(5.5%[5.0-5.9])。1990 年,主要风险因素是儿童发育不良(7.9%[6.8-9.4])、固体燃料产生的室内空气污染(HAP;7.0%[5.6-8.3%])和包括二手烟在内的烟草使用(6.1%[5.4-6.8%])。饮食风险因素和身体活动不足合计占 2010 年全球 DALY 的 10.0%(95%UI 9.2-10.8%),最显著的饮食风险因素是水果摄入量低和钠摄入量高的饮食。一些主要影响儿童传染病的风险因素,包括未改善的水和环境卫生以及儿童微量营养素缺乏,在 1990 年至 2010 年期间排名下降,未改善的水和环境卫生在 2010 年占全球 DALY 的 0.9%(0.4-1.6%)。然而,在撒哈拉以南非洲的大部分地区,儿童发育不良、HAP、非完全和中断母乳喂养在 2010 年仍是主要风险因素,而 HAP 是南亚的主要风险因素。2010 年东欧、拉丁美洲大部分地区和南撒哈拉非洲的主要风险因素是饮酒;在亚洲大部分地区、北非和中东以及中欧,主要风险因素是高血压。尽管有所下降,但包括二手烟在内的烟草使用仍然是北美和西欧高收入地区的主要风险因素。全球范围内的高体重指数有所增加,它是澳大拉西亚和南拉丁美洲的主要风险因素,在其他高收入地区、北非和中东以及大洋洲也排名很高。
在全球范围内,不同风险因素对疾病负担的贡献发生了重大变化,从儿童传染病风险转向成人非传染性疾病风险。这些变化与人口老龄化、5 岁以下儿童死亡率下降、死因构成变化以及风险因素暴露变化有关。新的证据导致了包括未改善的水和环境卫生、维生素 A 和锌缺乏以及环境颗粒物污染在内的关键风险因素的严重程度发生变化。流行病学转变的程度以及当前的主要风险因素在不同地区差异很大。在撒哈拉以南非洲的大部分地区,主要风险因素仍然是与贫困相关的风险因素以及影响儿童的风险因素。
比尔及梅琳达·盖茨基金会。