Department of Gastroenterology, Kitasato University School of Medicine, 2-1-1 Asamizodai, Minami, Sagamihara 252-0380, Japan.
Gastroenterol Res Pract. 2013;2013:192794. doi: 10.1155/2013/192794. Epub 2013 May 9.
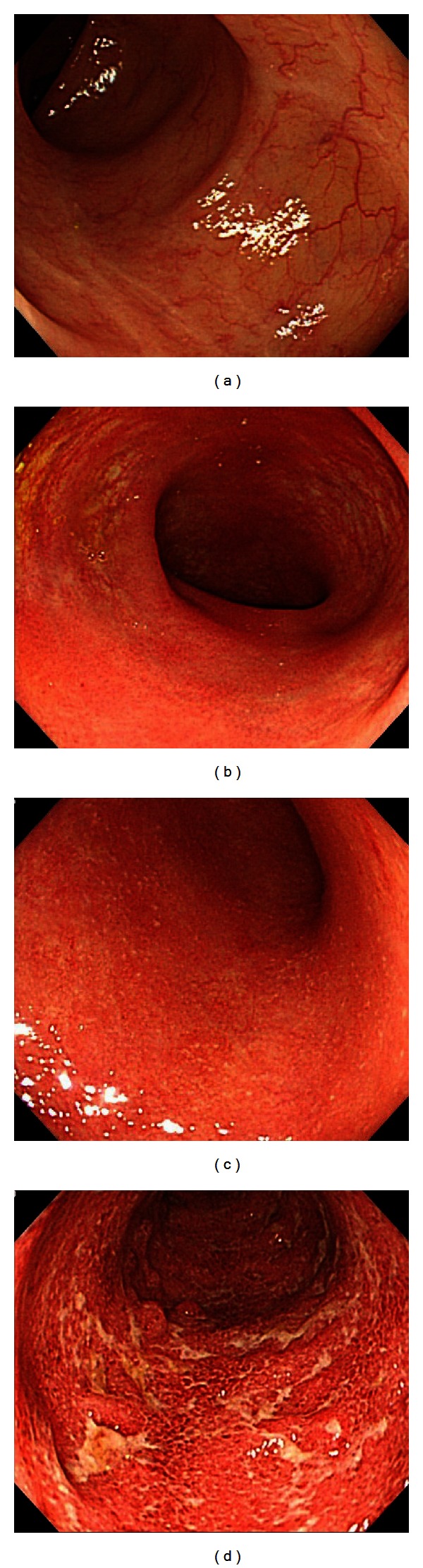
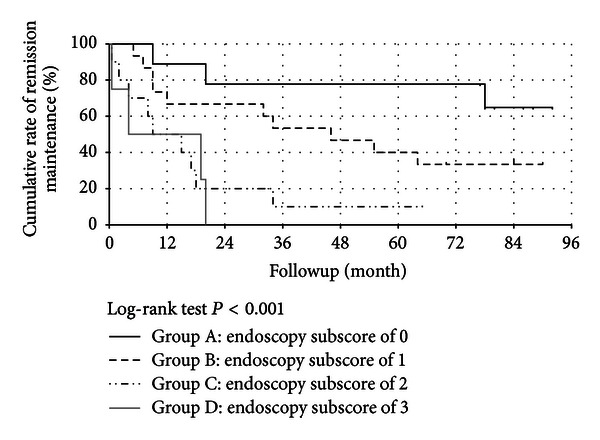
Background and Objectives. Mucosal healing (MH) is considered an important therapeutic goal in ulcerative colitis (UC). We evaluate the severity of intestinal inflammation and clarify the relation between MH and long-term outcomes. Methods. The study group comprised 38 patients with UC in clinical remission on total colonoscopy who were followed up for at least 5 years. Clinical remission was defined as a Mayo score of 0 for both stool frequency and rectal bleeding. Colonoscopic findings were evaluated into 4 grades according to the Mayo endoscopic subscore (MES). Results. During clinical remission, the MES was 0 in only 24% of the patients, 1 in 40%, 2 in 26%, and 3 in 10%. Seventy-six percent of the patients thus had active disease on colonoscopy. After initial colonoscopy, the cumulative rate of remission maintenance was 100% in MES 0, 1 in 93%, 2 in 70%, and 3 in 50% at 6 months and 78%, 40%, 10%, and 0%, respectively, at 5 years (P < 0.001). Conclusion. Many patients with UC in clinical remission have active lesions. Patients with a higher MES have a higher rate of recurrence. To improve long-term outcomes, an MES of 0 should be the treatment goal.
背景和目的。黏膜愈合(MH)被认为是溃疡性结肠炎(UC)的重要治疗目标。我们评估肠道炎症的严重程度,并阐明 MH 与长期结局的关系。
方法。研究组包括 38 例在全结肠镜下处于临床缓解期且至少随访 5 年的 UC 患者。临床缓解定义为粪便频率和直肠出血的 Mayo 评分均为 0。根据 Mayo 内镜评分(MES),内镜表现评估为 4 个等级。
结果。在临床缓解期,仅有 24%的患者 MES 为 0,40%为 1,26%为 2,10%为 3。因此,76%的患者在结肠镜下存在活动期疾病。初次结肠镜检查后,MES 0 的患者缓解维持率在 6 个月时为 100%,在 5 年时为 78%,MES 1 的患者缓解维持率在 6 个月时为 93%,在 5 年时为 40%,MES 2 的患者缓解维持率在 6 个月时为 70%,在 5 年时为 10%,MES 3 的患者缓解维持率在 6 个月时为 50%,在 5 年时为 0(P < 0.001)。
结论。许多处于临床缓解期的 UC 患者存在活动病变。MES 较高的患者复发率较高。为了改善长期结局,MES 为 0 应作为治疗目标。