Muhle Claus, Ahn Joong Mo, Dieke Constanze
Radiology Vechta, St. Marienhospital Vechta, Marienstr. 6-8, 49377 Vechta, Germany.
Springerplus. 2013 May 8;2(1):213. doi: 10.1186/2193-1801-2-213. Print 2013 Dec.
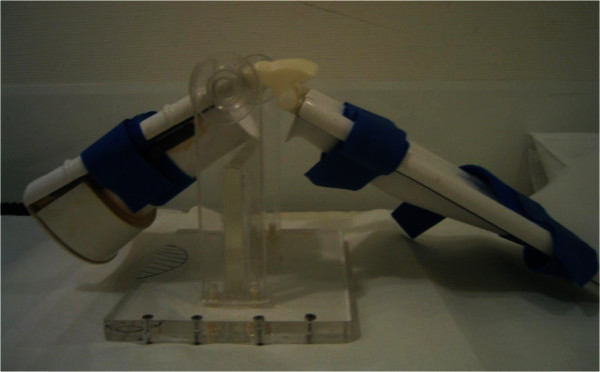
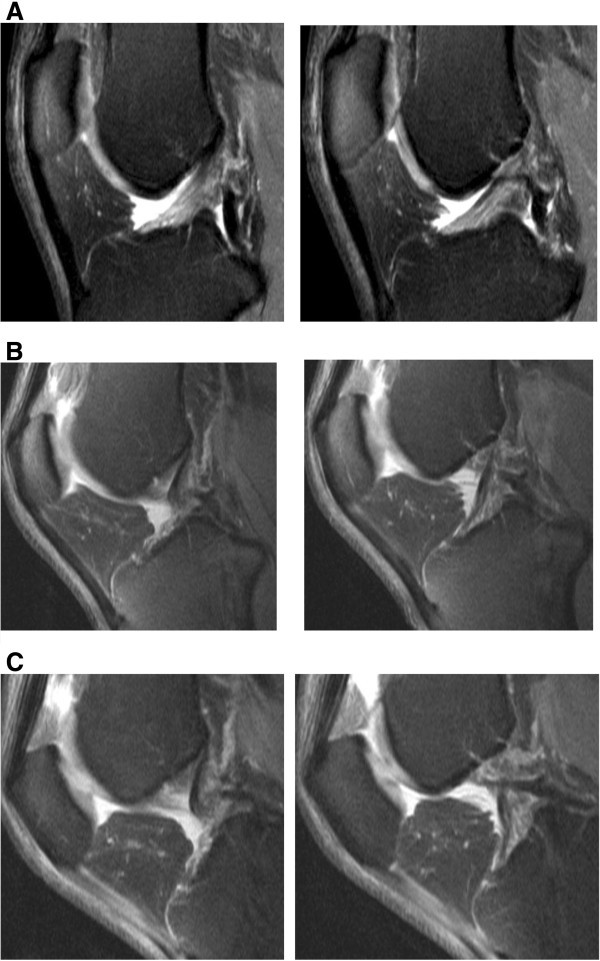
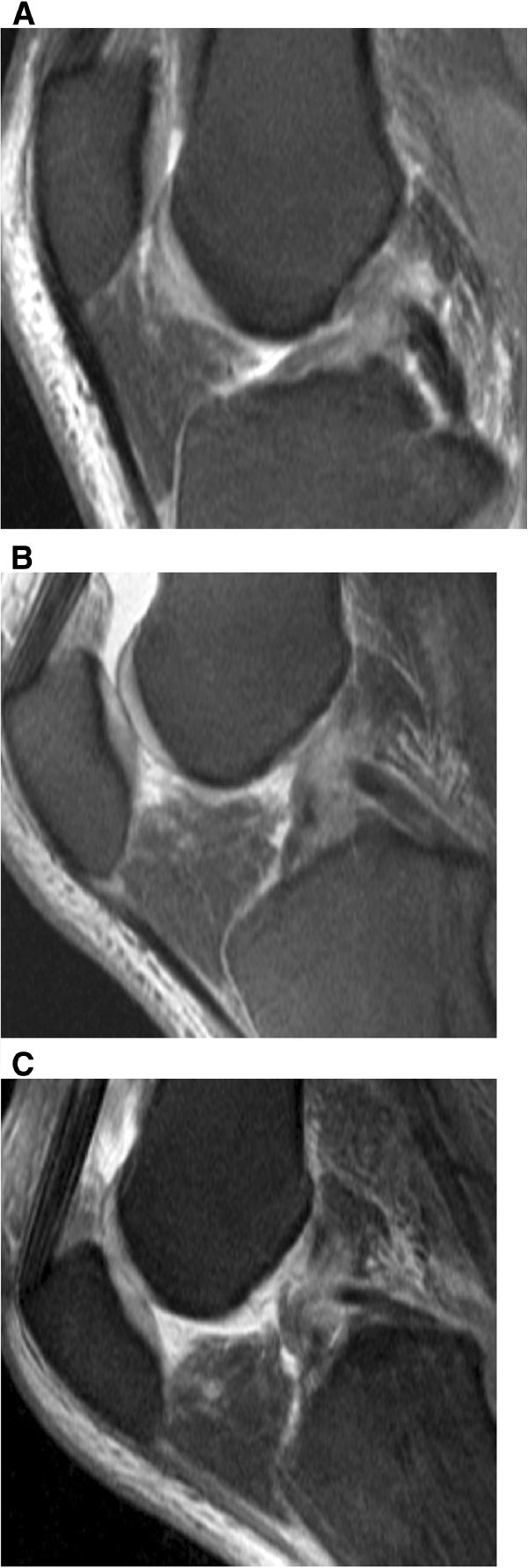
The aim of the study was to evaluate whether MR Imaging of the knee at 30° and 55° of flexion can improve the diagnosis of anterior cruciate ligament and menisci injuries compared to arthroscopy and imaging during extension of the knee joint. Knee joints from 40 patients with clinical suspicion of an anterior cruciate ligament (ACL) rupture were examined using MRI while the knee joint was either extended or flexed at 30° and 55° of knee flexion. A standard MR knee coil was used at extension, whereas at 30° and 55° of flexion a non-metallic positioning device and a flexible surface coil was placed ventral to the patella. Sagittal T2-weighted TSE sequences were acquired. In 29 of 40 patients, arthroscopy results were compared to the MRI examinations. Image quality of MRI examinations was evaluated using a three-point rating scale in a blinded fashion. Images were compared between groups and rated as better quality, same quality, or worse quality. Additionally, each angle MRI was compared to arthroscopy results. Partial ACL ruptures were diagnosed with 63% accuracy using MR imaging at 30° and 55° of knee flexion compared to 50% accuracy during knee extension. MRI imaging of complete ACL ruptures resulted in 83% accuracy of diagnosis when imaged at 30° flexion, 93% accuracy at 55° flexion, and 83% accuracy at extension. The accuracy of diagnosing medial meniscus lesions was 73% at extension, 64% at 30° flexion and 73% at 55° of flexion. MR imaging was only able to diagnose lateral meniscus tears with 55% accuracy in all three knee positions. The diagnosis of meniscal tears was more difficult due to small peripheral tears. The improved results in the diagnosis of ACL tears in response to 30° flexion and in particular in response to 55° flexion were based on the fact that the anterior cruciate ligament moved further away from the intercondylar roof with increased knee flexion. During flexion the ligament tension decreased, which causes the anterior cruciate ligament to have cylindrical shape and therefore made visualization of the injury easier. In conclusion, MR Imaging of the knee at 55° of flexion and less at 30° of flexion allows an improved diagnosis of injuries to the anterior cruciate ligament as compared to MRI examinations at extension. The diagnosis of meniscal injuries, however, was not superior at both flexion positions compared to commonly performed examinations at knee extension.
本研究的目的是评估膝关节在30°和55°屈曲位时的磁共振成像(MRI)与关节镜检查及膝关节伸展位成像相比,是否能改善前交叉韧带和半月板损伤的诊断。对40例临床怀疑前交叉韧带(ACL)断裂的患者的膝关节进行MRI检查,检查时膝关节处于伸展位或分别屈曲30°和55°。膝关节伸展位时使用标准的膝关节MRI线圈,而在屈曲30°和55°时,在髌骨前方放置一个非金属定位装置和一个柔性表面线圈。采集矢状面T2加权快速自旋回波序列。在40例患者中的29例中,将关节镜检查结果与MRI检查结果进行了比较。采用三点评分量表以盲法评估MRI检查的图像质量。对不同组的图像进行比较,并评为质量更好、质量相同或质量更差。此外,将每个角度的MRI与关节镜检查结果进行比较。与膝关节伸展位时50%的准确率相比,膝关节在30°和55°屈曲位时采用MRI诊断部分ACL断裂的准确率为63%。完全ACL断裂的MRI成像在膝关节屈曲30°时诊断准确率为83%,屈曲55°时为93%,伸展位时为83%。诊断内侧半月板损伤在伸展位时的准确率为73%,屈曲30°时为64%,屈曲55°时为73%。在所有三个膝关节位置,MR成像诊断外侧半月板撕裂的准确率仅为55%。由于半月板周边小撕裂,半月板撕裂的诊断较为困难。在诊断ACL撕裂方面,30°屈曲尤其是55°屈曲时结果有所改善,这是基于随着膝关节屈曲增加,前交叉韧带与髁间顶的距离进一步增大这一事实。在屈曲过程中韧带张力降低,这使得前交叉韧带呈圆柱形,因此更容易观察到损伤情况。总之,与膝关节伸展位的MRI检查相比,膝关节在55°屈曲位及较少程度的30°屈曲位时的MRI检查能改善前交叉韧带损伤的诊断。然而,与膝关节伸展位的常规检查相比,在这两个屈曲位时半月板损伤的诊断并无优势。