Division of Cardiology, Tulane University School of Medicine, and Association of Black Cardiologists, Inc., 1430 Tulane Ave., SL-48, New Orleans, LA, 70112, USA,
Am J Cardiovasc Drugs. 2013 Oct;13(5):301-13. doi: 10.1007/s40256-013-0033-4.
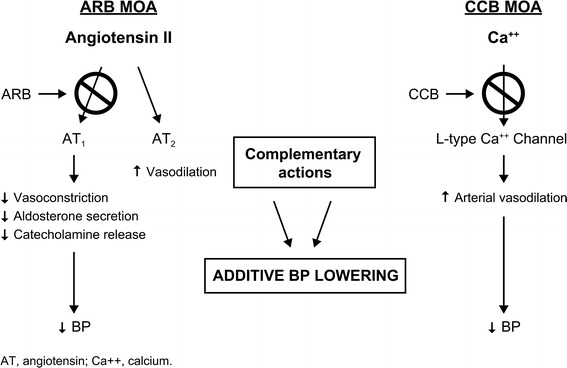
This article discusses racial/ethnic disparities in hypertension, with particular focus on non-white populations including blacks, Hispanics/Latinos, and Asians. Hypertension and its related morbidity and mortality affect a disproportionate number of black patients compared with white patients. Blacks, Hispanics/Latinos, and Asians have poor rates of hypertension awareness, treatment, and control. Given the high prevalence of comorbidities (e.g., obesity, diabetes, and metabolic syndrome) in these populations, renin-angiotensin-aldosterone system blockers are a good choice for foundation therapy. This review also discusses the importance of adherence and persistence with antihypertensive medication, which remain suboptimal in these non-white populations. Evidence suggests improvement with the use of single-pill combination therapy. Lastly, clinical trial data on the antihypertensive efficacy and safety of the combination of a dihydropyridine calcium channel blocker and an angiotensin receptor blocker, a widely utilized combination, in non-white populations are presented. PubMed was searched using the title/abstract key words (amlodipine AND valsartan AND [hypertension OR hypertensive] AND [black(s) OR African American(s) OR Hispanic(s) OR Latino(s) OR Mexican(s) OR Asian(s)]). In total, eight studies in patients with stage 1 or 2 hypertension were identified (n = 1,111 black, n = 389 Hispanic/Latino, and n = 3,094 Asian). Results showed that treatment with the combination of amlodipine plus valsartan is a reasonable choice for initial therapy or in patients who fail to respond to monotherapy. These drug classes have complementary mechanisms of action and, when used concomitantly, the magnitude of blood pressure lowering in these non-white populations is generally comparable with that seen in non-Hispanic white patients.
本文讨论了高血压中的种族/民族差异,特别关注包括黑人、西班牙裔/拉丁裔和亚洲人在内的非白人群体。与白人患者相比,高血压及其相关的发病率和死亡率对黑人患者的影响不成比例。黑人、西班牙裔/拉丁裔和亚洲人高血压知晓率、治疗率和控制率较低。鉴于这些人群中并存疾病(如肥胖、糖尿病和代谢综合征)的高发率,肾素-血管紧张素-醛固酮系统阻滞剂是基础治疗的不错选择。本文还讨论了坚持使用抗高血压药物的重要性,在这些非白人群体中,这方面仍不尽如人意。有证据表明,使用单片复方制剂治疗可有所改善。最后,本文介绍了在非白人群体中,二氢吡啶钙通道阻滞剂和血管紧张素受体阻滞剂联合使用的降压疗效和安全性的临床试验数据。在 PubMed 中使用标题/摘要关键字(氨氯地平 AND 缬沙坦 AND [高血压 OR 高血压性] AND [黑人 OR 非裔美国人 OR 西班牙裔 OR 拉丁裔 OR 墨西哥裔 OR 亚洲人])进行搜索。共确定了八项针对 1 期或 2 期高血压患者的研究(n = 1111 名黑人,n = 389 名西班牙裔/拉丁裔,n = 3094 名亚洲人)。结果表明,氨氯地平加缬沙坦联合治疗是初始治疗或单药治疗失败患者的合理选择。这些药物类别具有互补的作用机制,当联合使用时,这些非白人群体的血压降低幅度通常与非西班牙裔白人患者相似。